KEY ACTIVITY #3:
Use Care Gap Reports or Registries to Identify All Patients Eligible and Due for Care
This key activity involves all seven elements of person-centered population-based care: ooperationalize clinical guidelines; implement condition-specific registries; address social needs.
Overview
This foundational activity provides detailed guidance on how to reliably and efficiently develop and use a regularly updated list of patients eligible for recommended or standard screenings or interventions (e.g., blood pressure, lab work, etc.) through a care gap report or registry. Please note that this activity focuses on diabetes and hypertension; many other preventive and maintenance services are needed to provide comprehensive preventive care (see the Pre-Visit Planning: Leveraging the Team to Identify and Address Gaps in Care resource for a more complete list).
Care gaps are gaps between the recommended care that a patient should receive according to clinical guidelines and the care a patient actually receives.
Most EHRs already have a module that identifies what services are due for each patient (see examples below).
FIGURE 4: EXAMPLE OF A CARE GAP REPORT FOR AN INDIVIDUAL PATIENT (BLOOD PRESSURE)
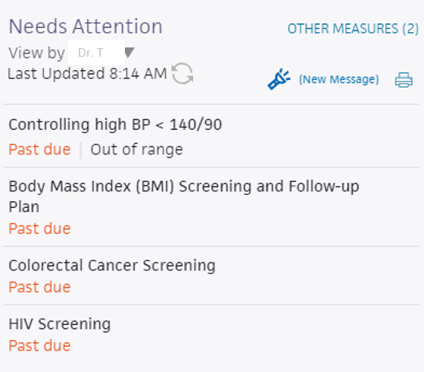
FIGURE 5: EXAMPLE OF A CARE GAP REPORT FOR AN INDIVIDUAL PATIENT (HEMOGLOBIN A1C)

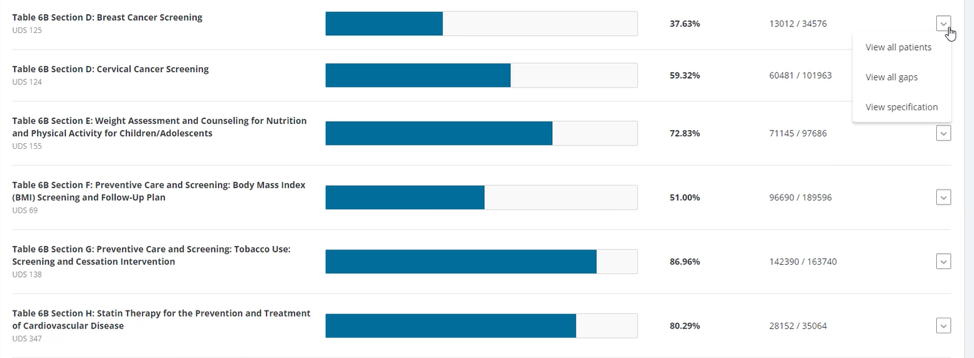
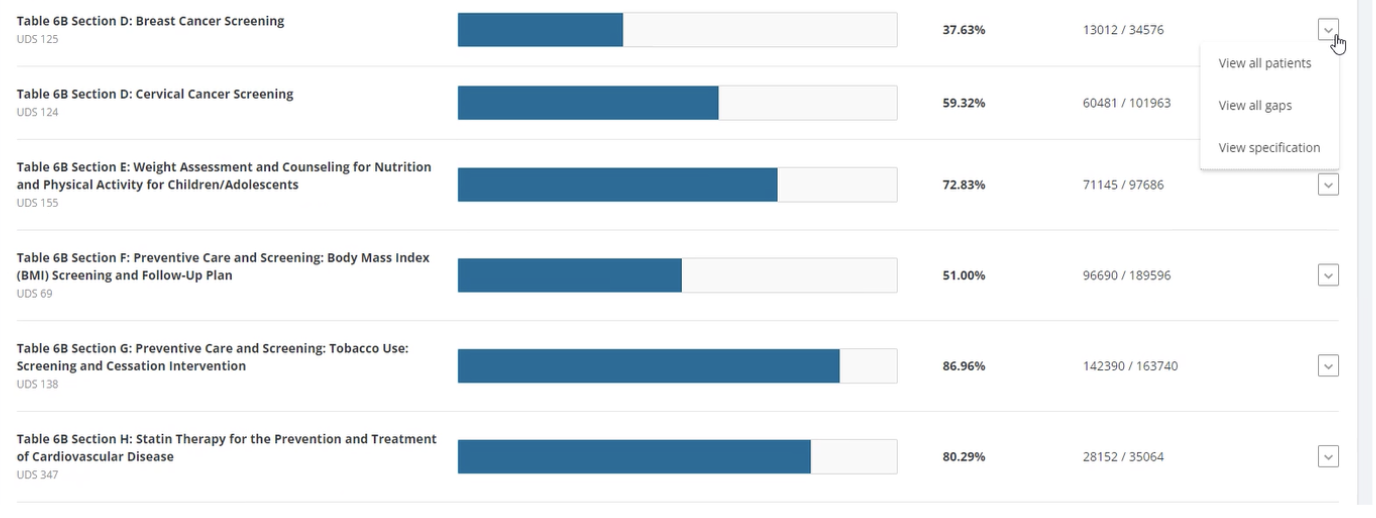
FIGURE 6: EXAMPLE OF A CARE GAP REPORT SUMMARY AT A POPULATION LEVEL
A registry is a list of patients with a specific characteristic that can be used for tracking aspects of screening, treatment or outcomes. At minimum, a registry should include:
- Medical record number. (MRN)
- Patient name.
- Date of birth.
- Contact information.
- Race, ethnicity, and preferred Language (REAL).
- SOGI data.
- Clinical data points that are being checked for care gaps.
An example chronic care registry report from the American Medical Association highlights clinical data points that may be important to consider when building a chronic care registry.
Care gap reports are reports embedded in EHRs that use the registry concept to identify patients assigned to your care team or in some other cohort, who have a specified care gap.
Rather than put the responsibility on an individual care team member for searching through charts or remembering which patients need further preventive care or follow-up, this key activity provides guidance on how the practice can efficiently leverage EHRs to identify patient care gaps.
Care gap reports are essential for practices to understand and continually improve consistency and reliability for meeting guidelines for preventive care and chronic disease management. At the care team level, care gap reports focus on gaps for patients assigned to your care team and help your team understand which patients you are responsible for. They can be used to:
- Support improvements to the pre-visit planning (PVP) process, standing orders and other routine clinical workflows designed to systematically identify and address gaps in recommended care.
- Prioritize patients to whom care teams should provide proactive outreach and reminders for engaging in care.
- Support quality improvement efforts with an equity lens.
- Improve your performance on key measures by ensuring you are able to do follow-up assessments/screenings for patients overdue for services (such as labs, ophthalmology checks for people with diabetes, foot screening for neuropathy, etc.).
Actively identifying and acting on care gaps ensures all eligible patients assigned to your practice receive timely screenings for chronic disease and other preventive services. This reduces the burden on the healthcare system by preventing more severe health issues in the future. Furthermore, this reduces missed or delayed diagnoses. For adults with chronic conditions, care gap reports can identify patients who are due for regular or infrequent required screenings in accordance with clinical care guidelines, including guidelines that may be established by specific payors. They also can identify opportunities for screening and improvement for controlling said chronic conditions.
Many practice patients experience barriers to accessing care due to structural and historical racism, homophobia, xenophobia and other biases that have historically disadvantaged individuals and groups from receiving equitable services. Defining clear criteria and gaps for patients due for specific screenings or preventive services helps to illuminate groups that have not had equitable access. It also combats biases by standardizing expectations for who is due for what care, providing a starting point for ensuring reliable and equitable access.
Staff can identify potential barriers and challenges for patients accessing and engaging in care by using enhanced care gap reports to filter and display the data alongside demographic information, social needs, behavioral health needs and communication preferences. This information can be used to promote a person-centered approach when designing the care plan, promoting self-care and conducting other patient engagement activities, such as conducting outreach in the patients’ preferred language.
Furthermore, care gap reports that segment the data into cohorts based on demographic and other personal information may help the team identify inequities in care, access and outcomes, which can inform improvement efforts. For example, therapeutic intensity requirements may differ by population. It is also important to gain input from the patient to ensure that their needs are being met.
Care gap reports can be used during pre-visit planning (PVP) to identify people for whom social needs screening has not yet been completed. This creates an opportunity to identify unmet social health needs and to connect patients with resources that address their social needs. See Key Activity 10: Develop or Refine and Implement a Pre-Visit Planning Process for more information.
Many EHRs already have a module that identifies what services are due for each patient whereas others do not. Where this functionality is available, it may not be configurable to align with the health center’s specific protocol or be able to incorporate outside data. Other options for developing registries include supplemental applications, population health platforms and freestanding customized databases that draw data from the EHR and other sources.
Care gap reports may be embedded in EHRs or made available through other technology channels (See Appendix E: Guidance on Technological Interventions.)
They are useful both at the individual patient level and aggregated to identify groups of patients to facilitate population-level management through registries.
A registry can be thought of as simply a list of patients sharing specific characteristics that can be used for tracking and management. Both care gap reports and registries should have the capacity to segment patients by age, gender, race/ethnicity and language.
Other relevant HIT capabilities to support/relate to this activity include care guidelines, care dashboards and reports, quality reports, outreach and engagement, and care management/care coordination.
(See Appendix E: Guidance on Technological Interventions.)
Access to outside data (e.g., California Immunization Registry/immunization data and data from other practices) may be a consideration or requirement as services received outside the practice may be part of compliance. While claims data may be helpful in this regard, lag time may impact its usefulness. Patient-facing applications should be strongly considered to ensure patients are informed and appreciative of the nature and importance of recommended care. In California, many healthcare organizations are required or have chosen to participate in the California Data Exchange Framework (DxF), which can facilitate data sharing between clinics, managed care plans (MCPs) and other partners.
Action steps and roles
1. Plan the care gap report.
Suggested team member(s) responsible: panel manager or data analyst. If it is not clear how the report can be produced, this step may involve one or more people from the practice who work on the EHR and possibly the EHR vendor.
As a team, decide what screenings or treatment guidelines are appropriate for your population of focus and prioritize the most important care gaps to run reports on. Start with the core and supplemental measures and any process measures your practice is tracking, then consider if there are any other gaps, clinical guidelines or measures your practice feels important to prioritize.
Identify the inclusion criteria for each report, such as age, any exclusion criteria and factors that make someone high risk.
Care gap reports should at minimum include monitoring for control of the following:
Among persons 18 to 75 years old with diabetes:
- No hemoglobin A1c test within the past six months.
- A1c >9% without a follow-up.
- Missing a urine albumin-to-creatinine ratio test in the past 12 months.
- Missing diabetic eye exam in the past 12 months.
- Missing diabetic foot exam in the past 12 months.
Among persons 18 to 85 years old with hypertension:
- No documentation of blood pressure in the past 12 months (or ever).
- If the last blood pressure was uncontrolled.
- If there was no documented follow-up if the blood pressure was elevated.
Care gap reports should also be developed to flag persons not meeting HEDIS measure thresholds who require follow-up because of positive screening results or lab values outside recommended limits. Many such reports may already be part of your clinic’s EHR.
2. Build the report.
Suggested team member(s) responsible: data analyst.
Determine whether the EHR has an existing report or one that can be modified to fit the inclusion criteria. You should talk to staff who are familiar with the electronic record; in some cases, it may be necessary to consult with the EHR vendor to confirm this information and how to run the report.
The care gap format should include:
- Criteria for inclusion in the report.
- The overall compliance rate for the care gap being measured.
- All patients eligible for the screening or intervention and their addresses and phone numbers.
- The last date the test was performed, if known or if applicable; the previous results; and the type of test used.
- Preferred method of communication (e.g., phone, email, text).
Reports should be able to display and/or disaggregate the data based on:
- Race, ethnicity, and language (REAL) as well as sexual orientation and gender identity (SOGI).
- Any known social or behavioral needs.
- Communication preferences or other preferences that would inform the screening modalities offered or treatment preferences, such as documented declination of prior screenings or medications.
- Data on any other characteristic, including insurance data, that could pose a barrier to completing screening or influence treatment choices.
Report developers should also work to allow for evaluation of data on a clinician panel, clinic unit, whole clinic and health system level.
3. Standardize the data format.
Suggested team member(s) responsible: panel manager or data analyst.
Standardizing the data format and where it is entered is critical to ensuring accuracy in the resultant report. Once you know that a report can be produced, understand the specific data elements that are needed to produce the reports.
Document how each data element must be entered into the EHR in order to populate the fields needed for reporting. In some cases, data on completion of screening must be entered by hand (e.g., when the test is performed by a lab that does not communicate with the legacy EHR). Doing this will require a decision on the part of the practice as a whole and may require staff training and reinforcement on an ongoing basis. Where issues or apparent confusion is identified, regular discussion at team huddles or staff meetings will help in maintaining a standard approach.
Tip: Assign responsibility for the initial review of the reports to confirm data integrity.
4. Develop workflows to improve patient screening and preventive care completion rates.
Suggested team member(s) responsible: panel manager, care team and EHR specialist (or equivalent).
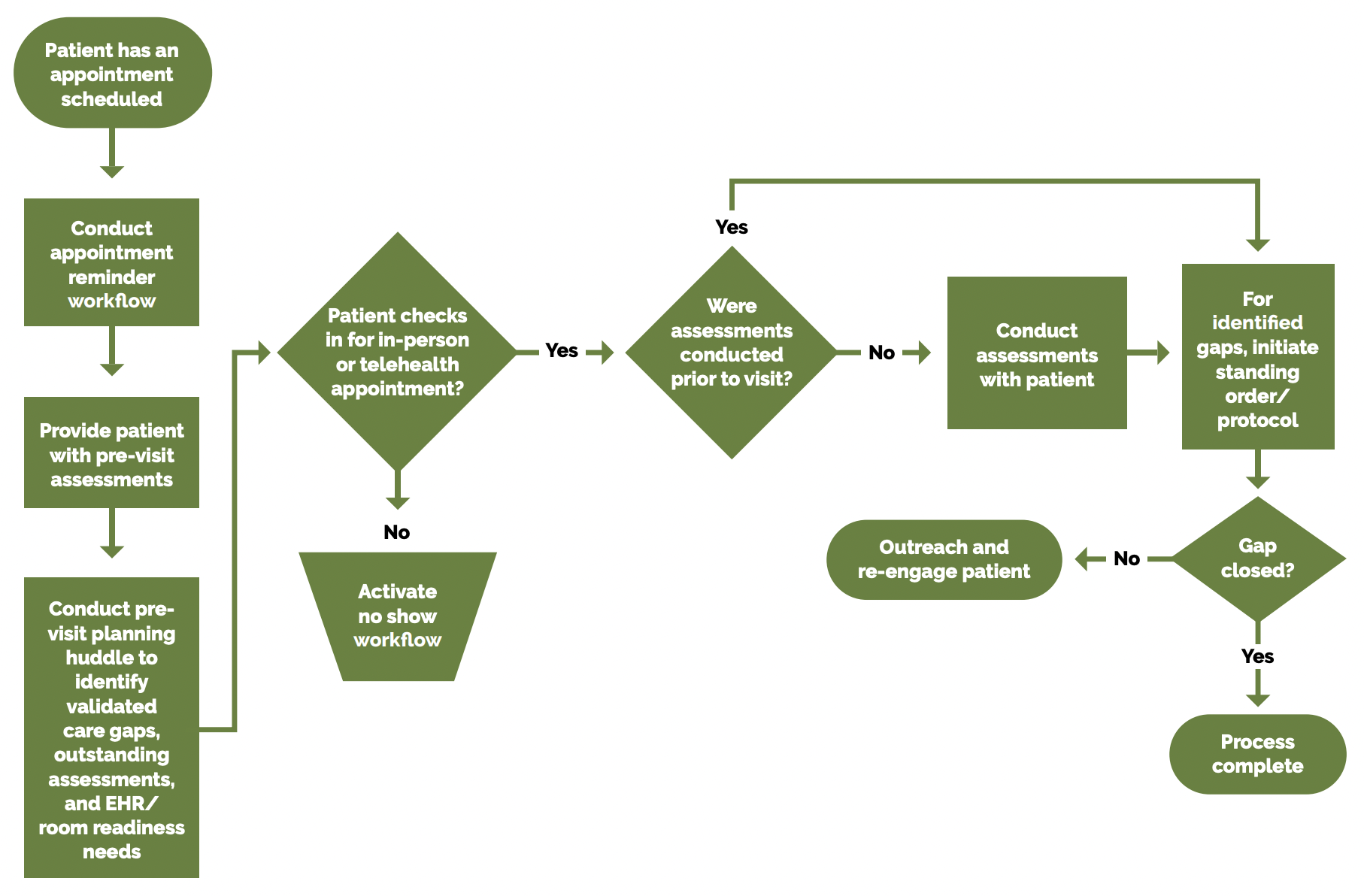
At the patient level, ensure that the care gap report can be used for or linked with reminders or alerts for clinicians, as well as for reminders to patients who need to come in to the clinic for screening or follow-up. As an example, a care gap report could alert the care team that a diabetic patient is in need of a foot check in accordance with the guidelines. For example, a standing order could trigger the MA who is trained in foot screening to do the foot check at the time of rooming. The workflow in Figure 7 applies to both chronic and preventive screening.
FIGURE 7: SCHEDULED PREVENTIVE CARE VISIT WORKFLOW
See the PHMI Care Teams and Workforce Guide Resource 6: Workflow Examples for more information.
Depending on communication preferences that have been expressed by patients, the patient care gap report may be exported to an automated reminder system that can trigger reminders by phone, text, email or postal mail.
In addition, as part of the practices’ PVP process, patient care gaps should be reviewed and flagged as part of the daily huddle. See Key Activity 10: Develop or Refine a Pre-Visit Planning Process for more details.
An example of this is the Axis Community Health project implemented through participation in the Population Health Learning Network. Axis Community Health wanted to improve its behavioral health data infrastructure to better track patient outcomes, adjust treatment and provide quality care. This case study describes the registry they created, key changes and outcomes.
5. Develop a process for reviewing gaps at the population level.
Suggested team member(s) responsible: panel manager.
Set a report frequency to review care gap reports at regular care team meetings or huddles in order to develop a plan for improvement at the population level. This may include an outreach campaign to build community awareness of the value of screenings and the availability of easily accessed screening services. Reports should be able to be drilled down to the clinician level for accountability and used by the care team to improve performance.
FIGURE 8: EXAMPLE OF A POPULATION CARE GAP REPORT DASHBOARD
Implementation tips
- Consider using other practice staff to help close gaps in care. For example, front office staff can assist with scheduling a follow-up nonacute visit to address gaps in care if a patient comes in for a sick visit.
- Consider incorporating chronic disease management into sick visits to further expand patients’ opportunity to receive care.
- Treatment intensity required for a patient can be benchmarked between providers in a practice. This can be accomplished by comparing treatment intensity rates over a period of time (i.e., three months), which can then be compared to the clinical effectiveness of interventions (i.e., diabetes control or hypertension control).
Resources
Evidence base for this activity
Conderino S, Bendik S, Richards TB, Pulgarin C, Chan PY, Townsend J, et al. The use of electronic health records to inform cancer surveillance efforts: a scoping review and test of indicators for public health surveillance of cancer prevention and control. BMC Medical Informatics and Decision Making. 2022 Apr 6;22(1).Sequist TD, Zaslavsky AM, Marshall R, Fletcher RH, Ayanian JZ. Patient and Physician Reminders to Promote Colorectal Cancer Screening. Archives of Internal Medicine. 2009 Feb 23;169(4):364.