Child Immunization Status
Well-Child Visits in First 30 Months of Life
The Population Health Management Initiative (PHMI) is working directly with a cohort of Community Health Centers to implement the latest population health management infrastructure. We are collaborating to improve the quality of care and address disparities for all patients and families served by California Community Health Centers.
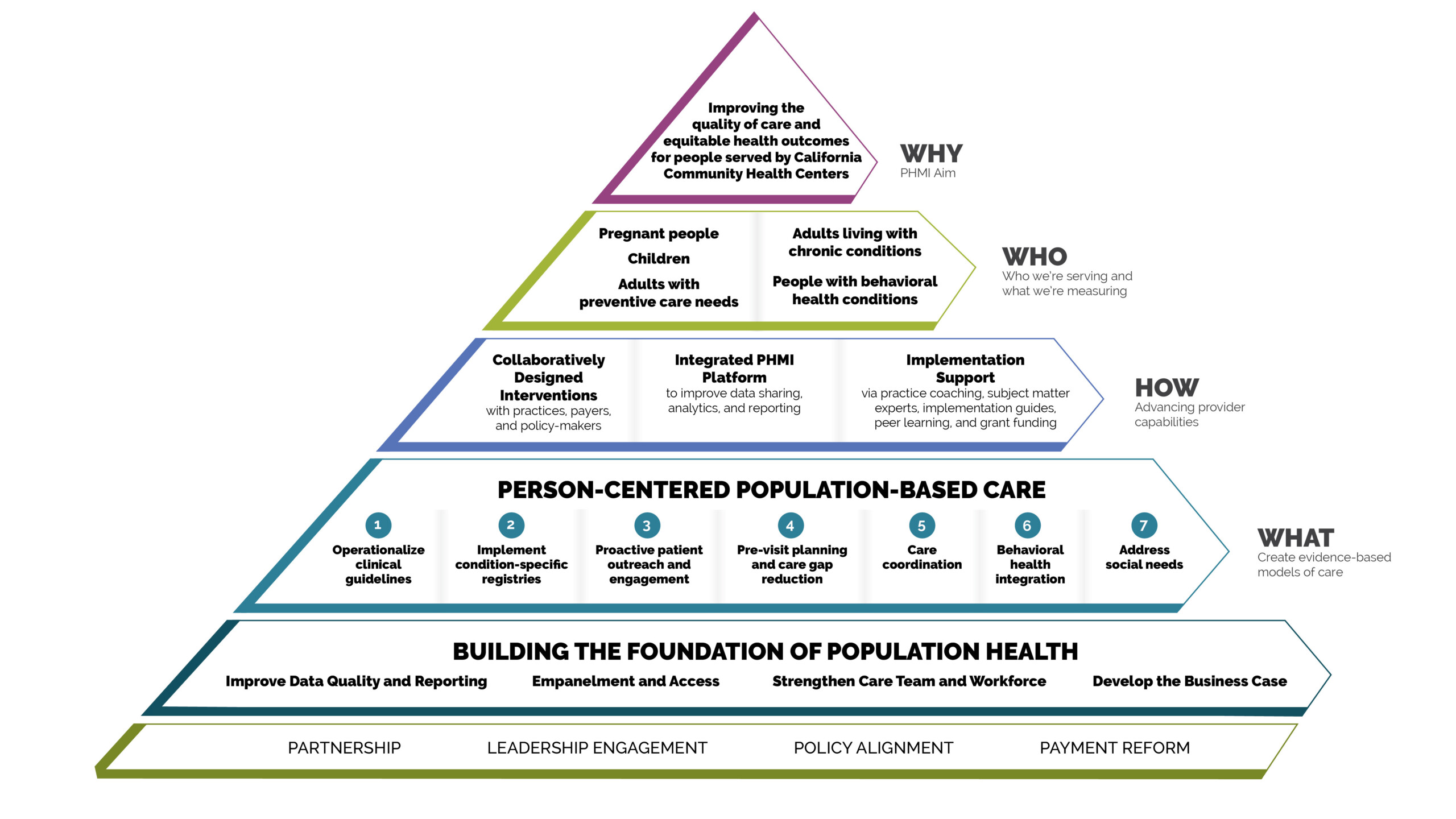
We worked together to identify key populations of focus and related measures of success. These measures are directly aligned with APM 2.0 to help organizations align payment structure with equity-based population health. Each Community Health Center has selected an area of focus and metrics that are most meaningful for the care they deliver and the people they serve.

Child Immunization Status
Well-Child Visits in First 30 Months of Life

Prenatal and Postpartum Care

Colorectal Cancer Screening

Controlling High Blood Pressure
Comprehensive Diabetes Care

Depression Screening and Follow-Up for Adolescents and Adults

Leaders from Community Health Centers, Regional Associations of California, California Primary Care Association, Department of Health Care Services, and Kaiser Permanente came together for interactive sessions to collaboratively align on the Population Health Management Initiative, think through ideal future state experiences for patients and care team members, and brainstorm solution concepts to consider for detailed design of the PHMI change package.
Based on the collaborative design process with Community Health Centers, two phases of implementation and a set of implementation supports emerged:
Community Health Centers will lay the groundwork to effectively implement population health management (PHM) for a selected population.
Each Community Health Center will select a core PHMI Population of Focus and apply the following core interventions, including, but not limited to:
Kaiser Permanente is investing in Community Health Centers to ensure their success in PHMI implementation by offering:
The PHMI Platform is a technology solution that functions with existing Community Health Center (CHC) technologies, enabling them to improve care quality and equitable health outcomes. It supports CHC and PHMI goals by:

Aggregating data from multiple sources to provide actionable analytics and better inform whole-person care
Strengthening and automating care management, physician engagement, patient outreach, and reporting workflows
Preparing CHCs for participation in CalAIM, APM 2.0, and value-based care
Building a foundation for statewide data aggregation, with the goal of enhancing data-sharing capabilities across the Medi-Cal delivery system
The Population Health Management Initiative is a five-year program to collaboratively design population health management strategies to advance provider capabilities and address disparities.
