KEY ACTIVITY #12:
Proactively Reach Out to Patients Due for Care
This key activity involves the following elements of person-centered population-based care: operationalize clinical guidelines; pre-visit planning and care gap reduction; behavioral health integration.
Overview
This activity provides guidance on how to effectively outreach to patients due for care. Proactive outreach can ensure patients follow through on recommended care. This is particularly important during pregnancy and postpartum when recommended care and referrals often are time-sensitive.
As part of pre-visit planning (PVP) and other clinical workflows, your practice should conduct some level of outreach to provide patients with information they may need to prepare for upcoming visits or engage in follow-up care plans determined during the visit. In addition, most electronic health records (EHRs) can be integrated with an automated reminder system for upcoming appointments and for patients who appear to have gaps in care. Patient outreach also occurs as a part of Care coordination, especially around supporting patients to engage in external referrals and in follow-up to a hospital admission or discharge. See Key Activity 13: Coordinate Care for further guidance.
Proactive outreach focuses on identifying subpopulations among patients who may benefit from additional outreach and implementing more personalized reminders and “touches” for them to engage in care.
Outreach to people who are not yet actively engaged in care goes beyond this foundational activity. See the "Going Deeper” Key Activity 18: Strengthen Community Partnerships for more about identifying trusted messengers in your community
Proactive outreach supports patients to remain engaged in care. It provides an opportunity for health needs to be identified and for patients to connect to appropriate care in a timely manner. As untreated health needs can lead to worse outcomes, proactive outreach may improve health outcomes. In the context of prenatal care, proactive outreach can identify missed appointments with specialists, ultrasounds needing to be completed, lab results missing from a patient’s chart or patients who have been out of care for extended periods of time. Because there is often two to four weeks between clinical visits during pregnancy, outreach interventions can ensure timely completion of important prenatal care testing and imaging.
Focus on equity by using data to identify which populations, subpopulations or groups the current outreach and education efforts don't reach. See the PHMI Data Quality and Reporting Guide for more information.
Co-designing outreach strategies with community partners and current patients promotes cultural humility and sensitivity. Tailored outreach with personalized reminders addresses diverse needs, reducing disparities in access to care.
Health-related social needs (e.g., income insecurity, transportation issues and health literacy) can result in no-shows and deterioration of patient health status. Proactive outreach, coupled with awareness of clues to health-related social needs, can connect patients to community resources and help to establish trust in the care team.
This activity relies on similar capabilities as care gap management, utilizing population views and registries to track prenatal care gaps against screening guidelines. These registries can be utilized to generate outreach lists for appointment schedulers and/or care managers and other care team members who might be tasked with contacting patients due for services. Many EHRs are capable of storing next appointment data that can also be used to generate lists, and may link to automated appointment outreach workflows. Patient-facing outreach and engagement technologies can be utilized to deliver appointment reminders and for patient self-scheduling. Care managers might use care management applications to track and prompt prenatal care needs, as well as postpartum visits.
Action steps and roles
1. Identify subpopulations among your obstetric patients who may benefit from outreach.
Suggested team member(s) responsible: Panel manager or data analyst with care teams.
- Start with frequent no-show patients and seek to understand their root causes, which may be related to social health-related needs or health literacy issues.
- Ask your care teams to identify patients they consider high-risk patients who have been lost to care.
- Use care gap reports to identify patients who are behind on prenatal testing or imaging or who have missed multiple prenatal visits. Patients who are engaged in care may still need additional care coordination or support. See Key Activity 3: Use Care Gap Reports or Registries to Identify All Patients Eligible and Due for Care for further guidance.
2. Establish the outreach model for your practice.
Suggested team member(s) responsible: Practice leadership.
One outreach model commonly used is to hire dedicated staff as population health specialists. This person would be responsible for using care gap reports to conduct proactive outreach to patients and schedule needed follow-up. See more about this in the care team duties and recommended education resource.
However, different teams may adjust this role to fit their context. An alternative model ensures each care team includes staff with knowledge of the local environment and available resources. These team members conduct telephonic outreach to higher needs patients and their families.
Train all outreach staff in cultural humility, motivational interviewing skills, and in the use of trauma-informed care.
3. Supplement your reminder system for contacting various subpopulations.
Suggested team member(s) responsible: Population health specialist with guidance from implementation team and IT staff.
Reminders should be sent to all persons with an upcoming scheduled appointment. The clinic scheduling system will likely have a function for generating automated reminders with an option for patients to cancel or reschedule if they cannot keep the appointment. Reminders should also be sent to all patients who appear to have gaps in care and missed appointments. See more in Key Activity 3: Use Care Gap Reports or Registries to Identify all Patients Eligible and Due for Care about updating your care gap reports to enable setting up automated reminders.
Automated reminder systems can support efficiency and reliability. However, more intensive reminders where the patient receives a personalized telephone call from their care team may help patients who are at higher risks of nonattendance or being lost to care.[1]
FIGURE 16: PROACTIVE OUTREACH & ENGAGEMENT EXAMPLE
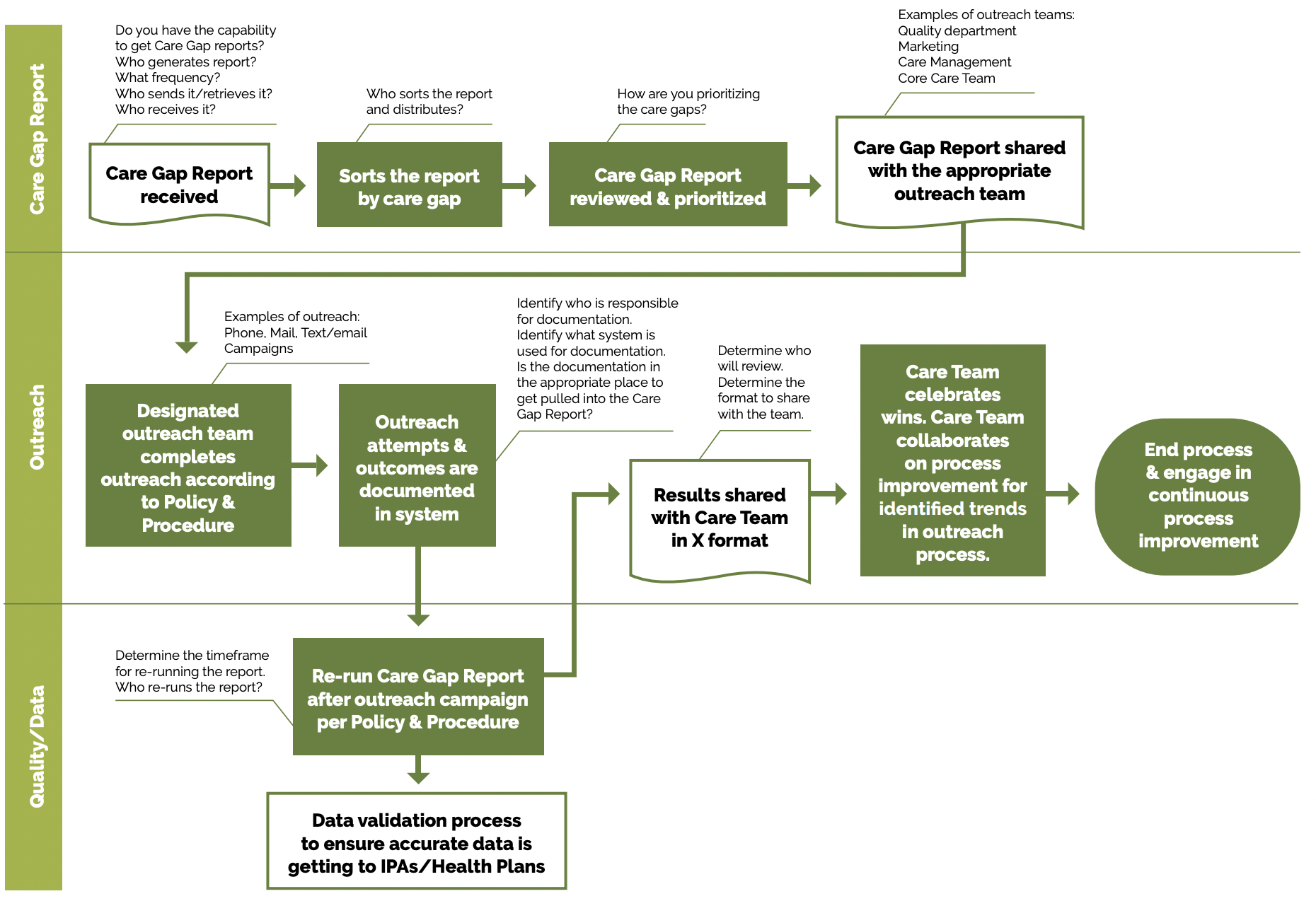
Utilize multiple pathways to reach and engage patients. For example, a Swiss clinic used sequential appointment reminders consisting first of a phone call and secondly of a text message if patients listed they received a postal reminder two days prior to their appointment. The reminder system significantly reduced the rate of missed appointments and allowed the clinic to reallocate 28% of the canceled appointments.[2]
Tip: Consider scheduling these outreached patients on days when you might experience a lower volume of activity in order to provide sufficient time for providers and staff to attend to the multiple patient needs that may be present.
Whether automated or manual, reminders should accommodate language requirements, as well as documented patient communication preferences (text, email, mail or phone). Reminders that include information beyond just the date, time and place may be more effective.[3] Consider including an orientation about what to expect and supporting clinical information.
4. Use “touches” that provide alternatives to the traditional office visit.
Suggested team member(s) responsible: Extended care team, including Enhanced Care Management (ECM), complex care management (CCM), community health workers, and population health specialist with guidance from implementation team.
Assess what types of interaction and care can be provided outside this setting, and collaborate with patients as part of initial care planning to understand their preferences for communication and care team interactions. Examples include, but are not limited to:
- Nursing visits (virtual).
- Pharmacy visits.
- Group prenatal care.
- Women, Infants and Children (WIC) program.
- Comprehensive Perinatal Support Services (CPSP).
- Black Infant Health (BIH).
- California Nurse-Family Partnership (NFP).
- Digital communication through emails, texts and patient portals.
- Newsletters focused on a specific condition.
- Social media that includes discussion groups relative to the management of conditions of focus.
- Home visits for high-risk, vulnerable or mobility-challenged patients.
- Other technological solutions, such as apps focused on patient conditions, which provide a vehicle for ongoing engagement.
5. Establish a process for engaging pregnant patients who have not yet been seen for prenatal care.
Suggested team member(s) responsible: Multidisciplinary implementation team.
It is important for practices to make a proactive plan to build capacity to accommodate pregnant-but-not-yet-seen patients in the clinic. Practices should develop strategies for outreach and engagement with these populations in order to shift them from not yet seen to fully engaged in prenatal care.
6. Continuously reassess outreach approaches with a goal of improvement.
Suggested team member(s) responsible: Population health specialist and ECM lead care managers.
- Test your co-designed outreach approaches and measure the effectiveness of your approaches. Review data (e.g., missed appointments, numbers lost to follow up, etc.).
- Survey patients to obtain retrospective and prospective feedback on outreach efforts.
- Engage ECM lead care managers to provide feedback on outreach efforts.
- Regularly update outreach strategies based on community feedback and changing demographics.
Evidence base for this activity
Biola H, Deyo J, Hayes T, Small L, Chaplin J, Pak-Harvey E, Granger T, Jung L, Fitzgerald L, Crowder C, Patel B, Stillwell T, Eisenson H, Granger B. Reaching the Hard-to-Reach: Outcomes of the Severe Hypertension Outreach Intervention. Am J Prev Med. 2020 Nov;59(5):725-732. doi: 10.1016/j.amepre.2020.05.030. Epub 2020 Oct 1. PMID: 33011006.
Denberg TD, Myers BA, Eckel RH, McDermott MT, Dickinson WP, Lin CT. A patient outreach program between visits improves diabetes care: a pilot study. Int J Qual Health Care. 2009 Apr;21(2):130-6. doi: 10.1093/intqhc/mzn060. Epub 2008 Dec 24. PMID: 19109334.
McLean SM, Booth A, Gee M, Salway S, Cobb M, Bhanbhro S, Nancarrow SA. Appointment reminder systems are effective but not optimal: results of a systematic review and evidence synthesis employing realist principles. Patient Prefer Adherence. 2016 Apr 4;10:479-99. doi: 10.2147/PPA.S93046. PMID: 27110102; PMCID: PMC4831598.
Endnotes
- McLean SM, Booth A, Gee M, Salway S, Cobb M, Bhanbhro S, Nancarrow SA. Appointment reminder systems are effective but not optimal: results of a systematic review and evidence synthesis employing realist principles. Patient Prefer Adherence. 2016 Apr 4;10:479-99. doi: 10.2147/PPA.S93046. PMID: 27110102; PMCID: PMC4831598.
- Perron NJ, Dao MD, Kossovsky MP, Miserez V, Chuard C, Calmy A, Gaspoz JM. Reduction of missed appointments at an urban primary care clinic: a randomised controlled study. BMC Fam Pract. 2010 Oct 25;11:79. doi: 10.1186/1471-2296-11-79. PMID: 20973950; PMCID: PMC2984453.
- McLean SM, Booth A, Gee M, Salway S, Cobb M, Bhanbhro S, Nancarrow SA. Appointment reminder systems are effective but not optimal: results of a systematic review and evidence synthesis employing realist principles. Patient Prefer Adherence. 2016 Apr 4;10:479-99. doi: 10.2147/PPA.S93046. PMID: 27110102; PMCID: PMC4831598.