Populations of Focus
KEY ACTIVITY #10:
Partner with Patients to Discuss and Arrange Cancer Screening Test
This key activity involves the following elements of person-centered population-based care: operationalize clinical guidelines; pre-visit planning and care gap reduction; care coordination; proactive patient outreach and engagement; address social needs.
Overview
This activity provides guidance on how the practice’s care team will use patient visits scheduled for other reasons to discuss and educate patients on needed colorectal, breast and/or cervical cancer screening. It also provides guidance for setting up a cancer screening test for any patient eligible. This includes patients who agree to get screened during a patient visit, in response to a screening reminder, or in response to an outreach activity. This includes guidance on the following screening methods:
- Screening at the practice.
- Providing screening materials during the visit to take at home.
- Providing screening modalities outside of the practice (e.g., mailed FIT, self-referred mammogram, or setting up an appointment for colonoscopy).
- Utilizing community linkages for screening (e.g., providing patients with contact to a mammography center or an outpatient surgical center for colonoscopy or sigmoidoscopy).
Why this matters
Numerous studies[1] [2] have demonstrated that having a clinician discuss the need for cancer screening directly with a patient is among the most effective and efficient strategies to support fulfillment of screening recommendations for colorectal, breast and/or cervical cancer. Developing skills to enable these critical conversations will increase the likelihood of success. In addition, patient education, discussing the benefits and risks of cancer screening, and offering a choice of testing modalities, where feasible, have all demonstrated improvement in cancer screening rates.[3]
Discussions about cancer screening should also address concerns the patient has about engaging in screening activities so that these can be taken into consideration and addressed.
When patients agree to a screening test, immediate action to undertake the test improves the likelihood of completion. Based on the screening recommended, this may involve scheduling the screening with a testing center or providing materials to the patient at the point of care.
Leveraging this intervention to address social needs and equity
This activity includes tailored messaging and a choice in screening modalities, where feasible, to increase the likelihood that historically vulnerable populations who have had lower cancer screening rates, higher rates of certain cancers, and/or higher mortality rates, complete the recommended screening. Initiating a screening recommendation provides an opportunity for dialogue with patients that may uncover barriers to beliefs about screening and to the ability and interest in undergoing screening, including unmet social needs that may prevent screening. Clinicians should explain the risks and benefits of the test and have relevant educational materials available. Our guidance for this activity, therefore, includes assessing social needs and addressing them.
Technology considerations
As discussed in Key Activity 3: Use Care Gap Reports or Registries to Identify All Patients Due for Cancer Screening, Key Activity 6: Conduct Proactive Outreach to Patients Due for Screening, and Key Activity 7: Refine and Implement a Pre-Visit Planning Process, technology can support care teams in their efforts to address cancer screening. Each modality will draw upon similar technical enablers to facilitate cancer screening for adults. The format in which planning is done needs to consider the workflow and staffing model.
Also, as discussed elsewhere, linkage to other sources of screening or follow-up is ideally facilitated by direct data connection to EHR and care coordination applications to support referral and follow-up, but where this is not possible a more manual process ought to be accompanied by a registry like function. (See the next section.) Relevant HIT capabilities to support this activity include care guidelines, registries, clinical decision-making support, care dashboards and reports, outreach and engagement, and care management and care coordination.
Action steps and roles
1. Plan for the cancer screening.
Suggested team member(s) responsible: Multidisciplinary team for cancer screening.
Planning and preparation are covered in the following key activities:
- Key Activity 2: Develop or Update the Practice’s Cancer Screening Protocols.
- Key Activity 3: Use Care Gap Reports or Registries to Identify All Patients Due for Cancer Screening.
- Key Activity 5: Develop and Implement Standing Orders.
- Key Activity 7: Refine and Implement a Pre-Visit Planning Process.
2. Use pre-visit planning and/or huddles to initiate this process.
Suggested team member(s) responsible: Primary care provider (PCP) and medical assistant (MA) for each panel.
This process starts during daily pre-visit planning and huddles by identifying which patients will need a reminder about the need for cancer screening(s) and the plan for having this conversation during the patient visit, including who will initiate the conversation and when. Patients who are eligible for screening tests should be flagged so that the PCP recognizes the need for guidance and recommendation. For more information, see Key Activity 7: Refine and Implement a Pre-Visit Planning Process and PHMI Care Teams and Workforce Guide Resource 4: Daily Huddles Overview and Process.
3. During the patient visit, discuss the need for colorectal, breast and/or cervical cancer screening and the importance of the screening(s) with the patient.
Suggested team member(s) responsible: Designated care team member, based on pre-visit planning.
The designated care team member should initiate the conversation about the need for screening. Based on the patient's age, risk factors, and medical history, the care team member should explain the importance of cancer screening. Effective communication strategies include:
- Asking open-ended questions about the patient's health, well-being and health goals.
- Listening attentively to patient questions or reservations and providing accurate, empathic answers.
- Promoting shared decision-making with the patient.
This should be done in the preferred language of the patient, using interpretation services as needed. Use or adapt existing curricula, scripts, patient materials, visuals and/or videos to help patients understand the importance of cancer screening. See the resources for this activity below.
Differentiating Between Average and Elevated Risk for Cancer Screening
Preventive healthcare includes participation in select screening tests that have been shown to identify disease early—before symptoms develop—and when treatment is most likely to be effective. This guide addresses steps to support screening for patients at average risk for breast, cervical, and colorectal cancer. Those who are at average risk should be encouraged and supported to undergo screening tests at the frequency noted in the PHMI clinical guidelines.
Some people, however, are at elevated risk for certain types of cancer, and they should be screened using specific screening methodologies at intervals that may differ from routine screening. Those at elevated risk should not be advised to follow the routine screening guidance outlined in the Implementation Guides but should follow individualized screening guidance in accordance with their risk for a particular disease.
Conditions and circumstances that elevate a person’s risk may be related to the presence of signs or symptoms suggestive of cancer, a personal history of cancer or of pre-cancerous conditions, a close family member with a specific cancer or certain types of exposure. When determining if a person is at elevated risk, it is useful to review their health history and ask the following questions at regular intervals, because an individual’s risk status may change over time:
- Have you ever been diagnosed with breast/cervical/colorectal cancer or a precancerous condition?
- Do you have a first degree relative (biological parent or sibling) who has been diagnosed with cancer or a precancerous condition?
- Do you have a genetic marker or syndrome associated with higher cancer risk?
- Do you have any medical conditions that place you at higher risk for cancer (for example, Crohn’s disease increases the risk for CRC cancer)?
- Have you had exposure to drugs or radiation that might affect your risk for cancer?
If a patient is identified as having an elevated risk for breast, cervical, or colorectal cancer, the primary care provider should discuss this risk with the patient and advise the patient of the modified recommendations for persons at elevated risk.
For additional information concerning increased risk for breast cancer, review the following guidance:
- American Cancer Society Recommendations for the Early Detection of Breast Cancer
- US Preventive Services Task Force Full Recommendation for Breast Cancer Screening, Practice Considerations
For additional information concerning increased risk for cervical cancer, review the following guidance:
- US Preventive Services Task Force Cervical Cancer: Screening Recommendations, Clinical Considerations
- Cervical Cancer Screening for individuals at average risk: 2020 guideline update from the American Cancer Society
For additional information concerning increased risk for colorectal cancer, review the following guidance:
- US Preventive Services Task Force Recommendations for Colorectal Cancer: Screening, Practice Considerations
- American Cancer Society Guideline for Colorectal Cancer Screening
Guidance Provided by:
- Margaret Franckhauser, MS, MPH, RN
- Adults with Preventive Health Needs Subject Matter Expert
References:
- U.S. Preventive Services Task Force. U.S. Preventive Services Task Force [Internet]. www.uspreventiveservicestaskforce.org. U.S. Preventive Services Task Force; 2022 [cited 2024 Dec 9]. Available from: https://www.uspreventiveservicestaskforce.org/uspstf/
- American Cancer Society. Cancer Screening Guidelines | Detecting Cancer Early [Internet]. www.cancer.org. American Cancer Society; 2023 [cited 2024 Dec 9]. Available from: https://www.cancer.org/cancer/screening/american-cancer-society-guidelines-for-the-early-detection-of-cancer.html
4. As needed, discuss the benefits and potential risks of colorectal cancer, breast cancer and/or cervical cancer screening with the patient.
Suggested team member(s) responsible: Designated care team member, based on pre-visit planning.
Use or adapt existing curricula, scripts, patient materials, visuals and/or videos to help patients understand the benefits and potential risks of cancer screening. This can include any differences in benefits or risks for the choice of screening modalities appropriate for them.
See the resources for this activity section below.
5. Discuss the choice of screening modalities with the patient when this is an option, and allow patients to select their preferred method.
Suggested team member(s) responsible: Designated care team member, based on pre-visit planning.
Offering patients a choice in healthcare screening methods, where choices exist, can increase the rate of screening completion. For example, patients are less likely to undergo colorectal cancer screening if the primary care practitioner only recommends colonoscopy, but screening rates increase when the provider offers the option of at-home fecal testing. Offering patients a choice allows them to address barriers to care, such as transportation, time limitations, or fear of anesthesia. Offering options places the patient in a position of authority over their own care.
See the resources for this activity section below.
6. Discuss which screening is covered and any out-of-pocket costs for cancer screening with the patient.
Suggested team member(s) responsible: Designated care team member, based on pre-visit planning.
Helping ensure that the recommended screening(s) are covered or low-cost may involve working with the patient’s health insurer, if one exists, modifying the timing of the screening, and other strategies. For patients who are not on Medi-Cal, this may require exploration with the insurer to verify coverage. Use or adapt existing curricula, scripts, patient materials, visuals and/or videos to help patients understand what is covered and what the out-of-pocket costs are related to colorectal cancer screening. See the resources for this activity section below.
7. As needed, discuss barriers to screening with the patient.
Suggested team member(s) responsible: Designated care team member, based on pre-visit planning.
Many patients have barriers to screening. To help reduce barriers (e.g., transportation, mobility, instructions in their preferred language, etc.), have an open discussion with each patient to understand the barrier(s) and co-develop potential ways to address each barrier with the patient. After the discussion, document the barriers and any strategies to address them in the EHR.
The Community Guide, endorsed by the American Academy of Family Physicians (AAFP), discusses specific interventions that can address structural barriers to breast, colon and cervical cancer screening.
8. Provide or arrange for the selected cancer screening.
Suggested team member(s) responsible: Designated care team member, based upon the test and the practice’s standing orders.
This is always based on your practice’s clinical practice guidelines and cancer screening protocols (See Key Activity 2: Develop or Update the Practice’s Cancer Screening Protocols.)
- Based upon the screening indicated and the option selected by the patient, if choices are available, the appropriate care team member will implement the practice’s cancer screening protocol and standing orders.
- If the selected screening test can be done during the visit, the clinician will implement the screening process, such as a Pap smear or fecal testing.
- If the selected screening procedure is to be conducted by the patient at home using a self-collected sample (e.g., FIT kit), the clinician will explain and demonstrate the proper collection techniques and the process to return the specimen for testing.
- If the screening requires further appointments (e.g., mammogram, colonoscopy, Pap Smear), the medical assistant or appropriate care team member may schedule the patient in the practice or initiate the referral, per protocol, and schedule the necessary follow-up appointments or provide referrals using preestablished community linkages.
- If the screening test requires laboratory analysis (e.g., Pap smear, fecal testing), the clinician will explain when the patient can expect to receive the results and what to do next.
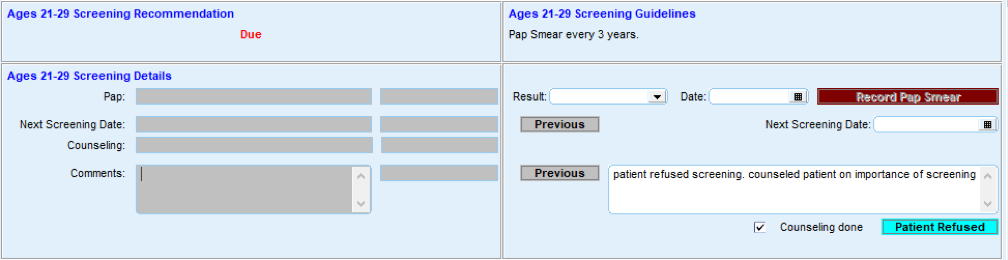
9. Document the screening.
Suggested team member(s) responsible: Medical assistant.
The medical assistant documents the cancer screening test(s) selected, including test type(s), date(s), and any relevant notes, in the patient's electronic health record (EHR).
FIGURE 21: EXAMPLE OF SCREENING DOCUMENTATION
10. Put in place formal and informal feedback loops with the care Team and patients.
Suggested team member(s) responsible: Panel manager and QI lead or their designee.
To help ensure this activity is meeting the needs of patients and is consistently feasible for the care team, it is important to have both formal and informal feedback loops.
For patients, feedback loops might include:
- Patient satisfaction surveys (or similar).
- Follow-up calls with a subset of patients to understand what went well and what could be improved.
- Patient focus groups.
- Having the practice’s patient advisory board (or similar) provide feedback.
For the care team, feedback loops might include:
- Existing or new staff satisfaction and feedback mechanisms.
- Regularly scheduled meetings and calls to get staff feedback on processes, methods and tools.
See also the Key Activity 9: Use Culturally Appropriate Educational Materials for Cancer Screening and Key Activity 10: Partner with Patients to Discuss and Arrange Cancer Screening Test for guidance on providing screening to patients who express interest in this.
11. Conduct ongoing quality assurance of the cancer screening process.
Suggested team member(s) responsible: QI lead or their designee(s).
The QI lead or their designee(s) should develop and implement a process to review a subset of records each month to ensure that this practice is in compliance with the practice’s cancer screening protocols, standing orders and any other of the practice’s relevant policies and procedures. In cases where policies and procedures are not being followed, the QI lead should initiate corrective action.
Sample workflow for colorectal cancer screen using FIT test:
- Assure that the patient is eligible for fecal-based testing by referencing your organization’s screening protocols outlined in Key Activity 2: Develop or Update the Practice’s Cancer Screening Protocols.
- Provide culturally and linguistically appropriate education materials and decision aides to the patient to ensure that they understand the benefits, risks and follow-up schedule for fecal-based testing (see Key Activity 9: Use Culturally Appropriate Educational Materials for Cancer Screening). Best practices include:
- Informing patients about the ability of different tests to detect colon cancer.
- Noting the frequency of each test type.
- Providing the patient with testing materials and instructions for the test of choice.
- Highlighting the time frame to return the sample.
- If the patient is available on site, review the sample procurement technique, return system and time frame with the patient while at the practice.
- Using culturally and linguistically appropriate materials and providing graphic diagrams where possible.
- If the patient is receiving the testing materials by mail, provide culturally and linguistically appropriate educational materials with an emphasis on graphic instructions and include information and materials for returning the test to the practice. Invite the patient to contact a specific person at the practice, if they have any questions.
- Document the delivery of materials for testing in the EHR.
- Process the sample or send the sample for processing within 24 hours of receipt and record the results in the EHR.
- Document results and instructions in the EHR. Assure that the EHR cancer screening report notes the patient as having received a fecal-based test in order for the eligibility roster to be generated in accordance with the USPSTF testing frequency guidelines.
- Contact the patient to inform them of the test results and the recommended follow-up (see Key Activity 11: Develop and Implement a Follow-Up System for Those Who Have Been Screened).
- If the patient cannot be reached to communicate positive test results, the team should design and implement alternative methods to reach patients, such as deploying community health workers to attempt to reach the patient and/or sending written communications.
Sample workflow for use of a mobile Pap screening clinic:
- Front office staff contact the patient by phone or in person to establish an appointment for a Pap smear and affirm the patient’s knowledge that the appointment is for the mobile unit. The front office staff confirm the patient’s understanding of the date and location of the appointment and how the mobile unit can be identified.
- Front office staff send the patient confirmation of the appointment by mail or text message with the date, time, and location and a reminder of the appearance of the mobile unit. They provide a number to call for questions or changes ahead of the appointment.
- The front office staff or mobile unit staff confirm the patient’s availability by text message the day before the appointment.
- At the mobile unit site, the clinical support personnel, such as an MA, greet the patient and invite the patient to enter the unit for pre-visit information gathering and confirmation of the appointment purpose and prepare the patient for the exam.
- The clinician conducts the exam, secures a Pap Smear, and addresses other clinical needs of the patient.
- The clinician and/or clinical support inform the patient of when the result is expected and how the patient will be informed of the result.
Implementation tips
- Consider how your existing technology can be leveraged to automate or partially automate the steps in this activity (e.g., EHR, automated survey mailers, email platforms, etc.).
- Where applicable, it is critically important to guide the patient in how to obtain and return the sample based on the type of test selected. Timing of the sample’s return is of the greatest importance and going outside the return time frame may render a sample to be invalid.
- Where multiple test modalities are offered, be sure to note the frequency of retesting, based on the method selected by the patient.
- Work with community representatives to develop messages and tools that are culturally relevant and understandable by the population.
- Combining clinician counseling and patient education materials improves patient likelihood of follow-through.
- Test each action, substep, or message on a small scale, ideally with community members, to identify challenges, ensure relevance and cultural accuracy, and refine before scaling up.
- Review the use of the testing materials while the patient is in the practice, if possible, and encourage them to ask questions and review the testing and return technique.
- Encourage patients to complete the test in a brief time frame so that it remains top of mind.
- See also Appendix D: Peer Examples and Stories from the Field to learn about how others are implementing this activity.
- See also Key Activity 3: Use Care Gap Reports or Registries to Identify All Patients Due for Cancer Screening for guidance on differentiating between average and elevated risk for cancer screening.
Resources
National Cancer Institute’s Cancer Screening Information - Patient Version
These web pages provide information that can be used or adapted for use with patients to explain the importance of screening and recommended tests available for:
Evidence base for this activity
Alberti LR, Garcia DP, Coelho DL, De Lima DC, Petroianu A. How to improve colon cancer screening rates. World J Gastrointest Oncol. 2015 Dec 15;7(12):484-91.
Dalton AF, Golin CE, Morris C, et al. Effect of a Patient Decision Aid on Preferences for Colorectal Cancer Screening Among Older Adults: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw Open. 2022;5(12):e2244982. doi:10.1001/jamanetworkopen.2022.44982.
Peterson EB. Ostroff JS, DuHamel KN, D’Agostino TA, Hernadez M, Canzona MR, Bylund CL. Impact of provider-patient communication on cancer screening adherence: A systematic review. Prev Med. 2016 Dec;93-96-105. Doi:10.1016/j.ypmed.2016.09.034. Epub 2016 Sep 28. PMID: 27687535; PMCID: PMC5518612.
Endnotes
- Alberti LR, Garcia DPC, Coelho DL, Lima DCAD, Petroianu A. How to improve colon cancer screening rates. World Journal of Gastrointestinal Oncology [Internet]. 2015;7(12):484. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4678395/
- Baron RC, Melillo S, Rimer BK, Coates RJ, Kerner J, Habarta N, et al. Intervention to Increase Recommendation and Delivery of Screening for Breast, Cervical, and Colorectal Cancers by Healthcare Providers. American Journal of Preventive Medicine. 2010 Jan;38(1):110–7.
- Peterson EB, Ostroff JS, DuHamel KN, D'Agostino TA, Hernandez M, Canzona MR, Bylund CL. Impact of provider-patient communication on cancer screening adherence: A systematic review. Prev Med. 2016 Dec;93:96-105.