Populations of Focus
Putting the Key Activities in Context
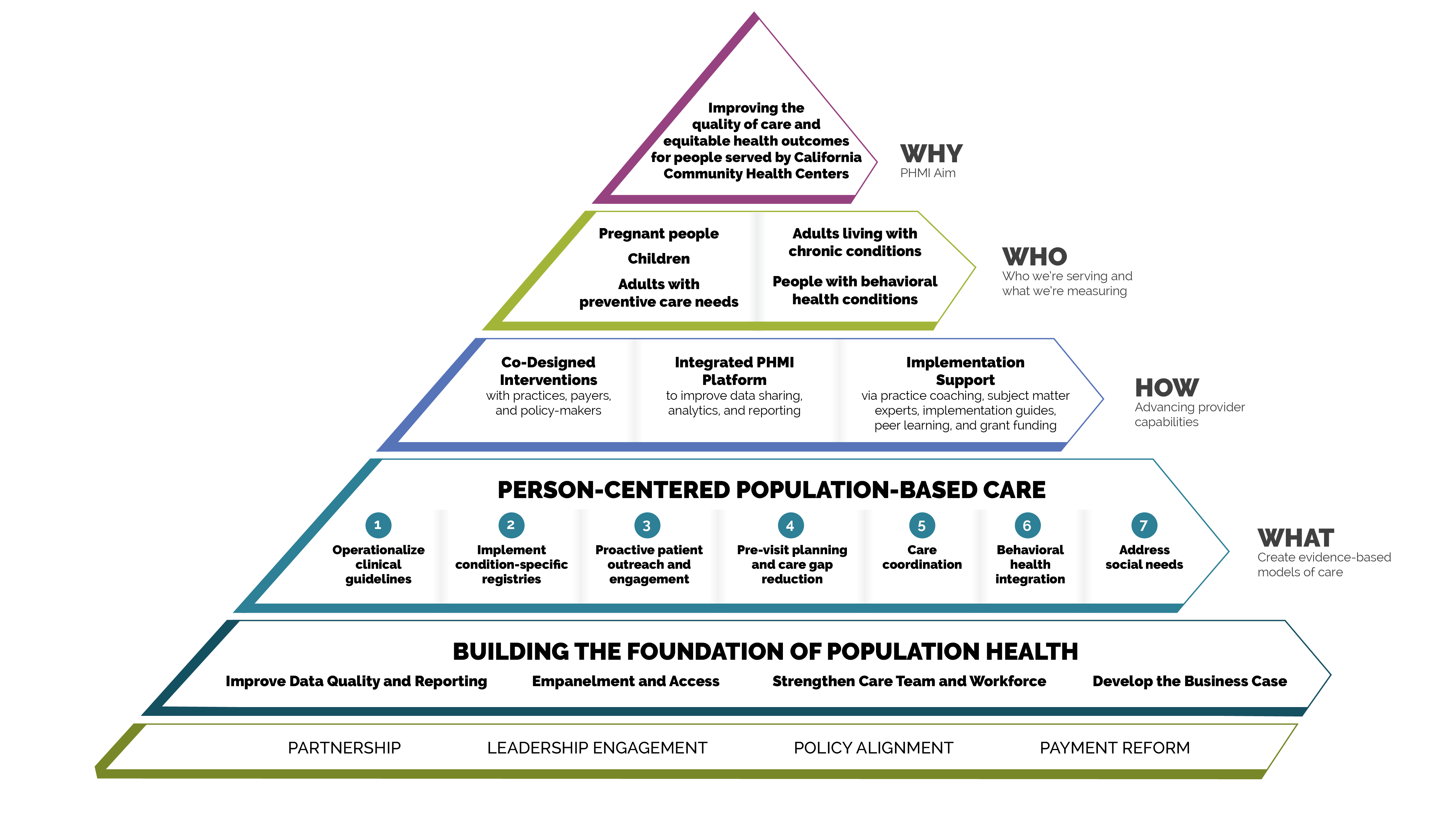
Person-centered population-based care
Each of the key activities advance one or more of the seven person-centered population-based care change concepts:
- Operationalize clinical guidelines.
- Implement condition-specific registries.
- Proactive patient outreach and engagement.
- Pre-visit planning and care gap reduction.
- Care coordination.
- Behavioral health integration.
- Address social needs.
FIGURE 1: PHMI IMPLEMENTATION MODEL
Core and supplemental measures
The measures covered in this guide consist of Healthcare Effective Data and Information Set (HEDIS) measures designated as core and supplemental measures by PHMI. These measures can be considered outcome measures because there is ample evidence that improved timely care will improve overall population health outcomes for adults requiring cancer screening. All measures use standard HEDIS definitions and are aligned with California Advancing and Innovating Medi-Cal (CalAIM) and Alternative Payment Methodology (APM) 2.0. For information about these measures, reference the PHMI Data Quality and Reporting Guide.
PHMI has selected one core and two supplemental measures of focus for adults with preventive care needs. Practices can track other measures that feel important and relevant. This guide provides detailed guidance to improve your practice’s results on the following four core and supplemental measures:
- Colorectal Cancer Screening (Core Measure).
- Breast Cancer Screening (Supplemental Measure).
- Cervical Cancer Screening (Supplemental Measure).
Core HEDIS measures for PHMI
|
PHMI Populations of Focus |
Measures |
|---|---|
Adults with preventive care needs |
Colorectal Cancer Screening |
Supplemental HEDIS measures for PHMI
|
PHMI Populations of Focus |
Measures |
|---|---|
Adults with preventive care needs |
Breast Cancer Screening |
|
Cervical Cancer Screening
|
Measurement strategy and learning system
The core and supplemental measures are part of a larger measurement strategy and learning system, as outlined in Appendix A: Sample, Idealized System Diagram: Weaving Your Measurement Strategy and Learning System into Practice Operations. Key Activity 1: Convening a Multidisciplinary Implementation Team for Cancer Screening outlines how your practice can develop a robust measurement system to support this work. In addition to quality assurance and monitoring, measures are also used during practice operations alongside other data for learning to:
- Guide the actions of the multidisciplinary implementation team as they use a systematic approach to decreasing inequities and implementing key activities across the practice.
- Support the care team’s efforts to advance population health and reduce care gaps through daily, weekly and monthly workflows, as well as continuous identification of opportunities for improvement.
Clinical practice guidelines
The PHMI Clinical Guidelines Advisory Group (CGAG) was established to create a standardized approach to review, adopt and promote established clinical guidelines in the PHMI cohort. For more information, please see the PHMI Clinical Practice Guidelines for Key Medi-Cal Populations of Focus.
Colorectal cancer screening clinical guidelines
FIGURE 2: CLINICAL GUIDELINES: COLORECTAL CANCER SCREENING
Guideline source |
|
PHMI measure |
Colorectal Cancer Screening |
Guideline language |
Conduct colorectal cancer screening for persons aged 45 to 75 using any of the following screening modalities and intervals:
|
Breast cancer screening clinical guidelines
FIGURE 3: CLINICAL GUIDELINES: BREAST CANCER SCREENING
Guideline Source |
|
PHMI Measure |
Breast Cancer Screening |
Guideline Language |
Age to start Mammography (USPSTF): Biennial screening mammography is recommended for women aged 40 y/o. The decision to start screening mammography in women prior to age 40 y/o should be an individual one. |
Cervical cancer screening clinical guidelines
FIGURE 4: CLINICAL GUIDELINES: CERVICAL CANCER SCREENING
Guideline Source |
|
PHMI Measure |
Cervical Cancer Screening |
Guideline Language |
Age 21-65 (USPSTF):
No Testing (USPSTF):
|
Utilizing this guide to improve equitable outcomes
Many key activities in this guide include considerations for utilizing the intervention to improve equitable health outcomes and reduce the effects of racism, bias and discrimination. Key Activity 4: Use a Systematic Approach to Address Inequities within the Population of Focus describes key action steps for how to make an intentional and explicit effort to identify inequities, understand root causes and reduce those inequities.
This guide also offers resources for going deeper into organizational and ecosystem-level work to advance equitable outcomes through Key Activity 16: Strengthen a Culture of Equity. More information about this approach can be found in the PHMI Equity Framework and Approach.
Integrating behavioral health
Integrated behavioral health supports are important for adults, as behavioral health support is likely to boost health outcomes and enhance patients' quality of life. One foundational change is to ensure that the care team includes behavioral health staff as core members of the team; this is covered in detail in the Care Teams and Workforce Guide.
To learn more about strategies for behavioral health integration see Getting Started with Behavioral Health Integration and the PHMI Behavioral Health Guide Key Activity 2: Enhance the Culture of Integrated Behavioral Healthcare and Key Activity 3: Enhance Operational Integration of Behavioral Health.
We also offer a resource, Pre-Visit Planning: Leveraging the Team to Identify and Address Gaps in Care, that includes recommended behavioral health screenings.
Throughout the key activities in this guide, we have incorporated considerations for providing trauma-informed care in the approach to cancer screening. Trauma is recognized as a potential barrier to seeking or engaging in cancer screening activities. Activities involved in breast, colon and cervical cancer screening may serve as potential triggers associated with the original trauma and should be considered and addressed carefully by clinicians. This guide, therefore, includes a resource for Trauma-Informed Population Health Management. For additional information about managing behavioral health conditions beyond screening, please see the behavioral health implementation guide.
Utilizing this guide to attend to patients' social needs
For many key activities in this guide, we have highlighted considerations related to social needs at the individual or population level, such as expanding referral networks. Key Activity 8: Use Social Needs Screening to Inform Patient Treatment Plans can help practices better understand and support patient- and population-level needs. For Medi-Cal patients and families with high levels of social need, such as those experiencing homelessness, referrals to Enhanced Care Management (ECM) and Community Supports programs are available; see Key Activity 15: Provide Care Management for more.
For going deeper in this area, practices can see Key Activity 14: Continue to Develop Referral Relationships and Pathways for common social needs and Key Activity 13: Strengthen Community Partnerships to build upon the strengths, infrastructure and resources available in the community. More information about this dual patient- and population- level approach is available in the PHMI Social Health Framework and Approach.
Our theory of change
Our theory of change is that if practices implement the activities contained in this guide, it will lead to improved health and well-being outcomes among the adults served by practices. See Appendix B: Theory of Change for a suggested driver diagram.