©️ 2024 Kaiser Foundation Health Plan, Inc.
This guide provides step-by-step guidance for improving population-based care for pregnant people with the goal of supporting substantive cultural, technological, and process changes, focusing on prenatal and postpartum care, and prenatal and postpartum depression screening and follow-up.
This guide was designed as part of the Population Health Management Initiative (PHMI), a California collaboration of the Department of Health Care Services (DHCS), Kaiser Permanente and Community Health Centers. Much of the content is relevant and adaptable to primary care practices of all kinds working to improve the health of the populations they serve.
Why is this important?
Timeliness of prenatal and postpartum care is important because it can improve the health outcomes and well-being of both pregnant people and infants and their families. Prenatal care is the healthcare that someone receives during pregnancy, and postpartum care is the healthcare that someone receives for the 12 months after giving birth. Perinatal is a term often used to describe this time during and after birth. For the purposes of this guide, “pregnant people” refers to pregnant and postpartum individuals up to 12 months postpartum, which aligns with extended coverage for Medi-Cal eligibility up to 365 days postpartum as well as Department of Health Care Services, Birthing Care Pathway Initiative, Enhanced Care Management Birth Equity Population of Focus and transitional care services for pregnant and postpartum individuals up to 12 months postpartum.
According to the Centers for Disease Control (CDC), timely and adequate prenatal and postpartum care can prevent more than 80% of all pregnancy-related deaths, as well as reduce the risks of complications, infections and low birth weight.[1] Such adverse health outcomes are largely preventable, but are exacerbated by variation in quality healthcare, underlying chronic conditions, structural racism and implicit bias.[2] These factors disproportionately impact people from racial and ethnic minority groups.
Racial and ethnic disparities in maternal health outcomes persist and increase as women age, as reported by the CDC. As of 2021, non-Hispanic white pregnant people died from pregnancy-related causes at a rate of 26.6 per 100,000 live births, while Black pregnant people died at a rate of 69.9 per 100,000 live births. American Indian and Alaska Native pregnant people also have higher risk of maternal mortality than white pregnant people, according to the CDC.[3] A study of maternal mortality in California found that provider-dependent factors, such as delayed response to clinical warning signs, were the most common contributor to maternal deaths.[4] This is particularly disturbing given the racial disparities in providers ignoring or refusing requests for help from women of color. Prenatal and postpartum care can also provide essential information and support to pregnant people and their families, such as nutrition, breastfeeding, family planning and emotional well-being. By ensuring that people have access to equitable prenatal and postpartum care, we can improve the health outcomes and quality of life for pregnant people and infants.
How to use this guide
The work to ensure that pregnant people receive all recommended care is a continuous effort and we still have much to learn. This “living” document uses existing evidence, bright spots and examples from the field to offer practical guidance on improving care for pregnant people. While some of the guidance in this document is technical, much of the guide focuses on supporting practices in the substantive cultural, technological and process changes that lead to improved population-based care for pregnant people. Virtually every activity in the guide will require some level of adaptation for your practice’s unique context. Population Health Management Initiative (PHMI) will update this guide as we learn from and with practices.
We have organized the key activities in this guide into three categories:
- Foundational activities: Activities that all practices should implement as part of their prenatal and postpartum care protocol.
- Going deeper activities: More advanced activities that build off of the foundational activities and that help ensure your practice can achieve equitable improvement in your prenatal and postpartum care.
- On the horizon activities: Additional activities, including ideas worthy of testing that include the latest ideas and thinking on prenatal and postpartum care.
Sequencing activities: We recommend that practices consider planning and attempting to implement the activities in the sequence provided in this guide. At the same time, we recognize that different practices may follow a different path toward prioritizing and implementing these activities. Furthermore, there is overlap between activities; many activities build off of or from the building blocks of other activities.
Testing and implementing: For each activity we provide guidance on how to plan, test and implement the activity along with links to other resources, technology considerations and examples. Consider testing different versions of the action steps and roles on a small scale before fully implementing at your practice.
Maintaining the progress: For many activities we have provided tips for periodically reviewing and making improvements to key workflows even after initially implementing the change. Ongoing review and continual improvement is important for your practice to maintain your progress in population health management and help you stay nimble in adapting to changing patient demographics, new clinical best practices, new payment policies, workforce changes and other changes at your practice.
If you implement the activities in this guide, you should be able to achieve the following foundational competencies:
For pregnant people, your practice will be able to consistently:
- Engage patients served by your practice to validate any of your proposed process improvements and to propose alternative methods to improve quality in your focus area.
- Analyze core and supplemental quality measures to identify improvement opportunities for achieving timely access to prenatal and postpartum care for attributed patients. Ensure that any analyses of your quality measures are stratified by key patient demographic characteristics to identify disparities in quality performance for specific attention.
- Use care gap reports or registries to identify all prenatal and postpartum patients due for care.
- Develop a process for screening pregnant and postpartum people for depression using evidence-based tools.
- Integrate behavioral health follow-up services as needed (e.g., for positive depression screens).
- Create an outreach protocol to reach and engage all attributed patients due for care.
- Create a health-related social needs screening process that informs patient treatment plans.
- Assess current capabilities and develop a plan for ongoing improvement in data utilization, care team workflows and efficiency that includes sustainable health information technology (HIT) strategies and continuous staff training on technology.
This guide also includes sections on measurement, equity, social health and behavioral health integration and an appendix including helpful tools and resources. We have included information about California Medi-Cal-covered benefits and services that were up to date at the time of publishing, but benefits and billing guidance change over time. Nothing in this guide should be considered formal guidance and anyone using this guide should check with the appropriate authorities on benefits and billing guidance. This document will be refined based on continued learning on this topic and may include additional activities, examples, resources and sections in the future.
Who is the audience for this guide?
Improving the health of a population impacts everyone in a practice. Critical roles needed to engage in the work outlined in this guide and support practice change include:
- Quality improvement leadership, like a director of quality improvement (QI), to support cultural changes.
- Coaches or practice facilitators who are partnered with teams to help identify areas for improvement and support change through change management strategies.
Putting the Key Activities in Context
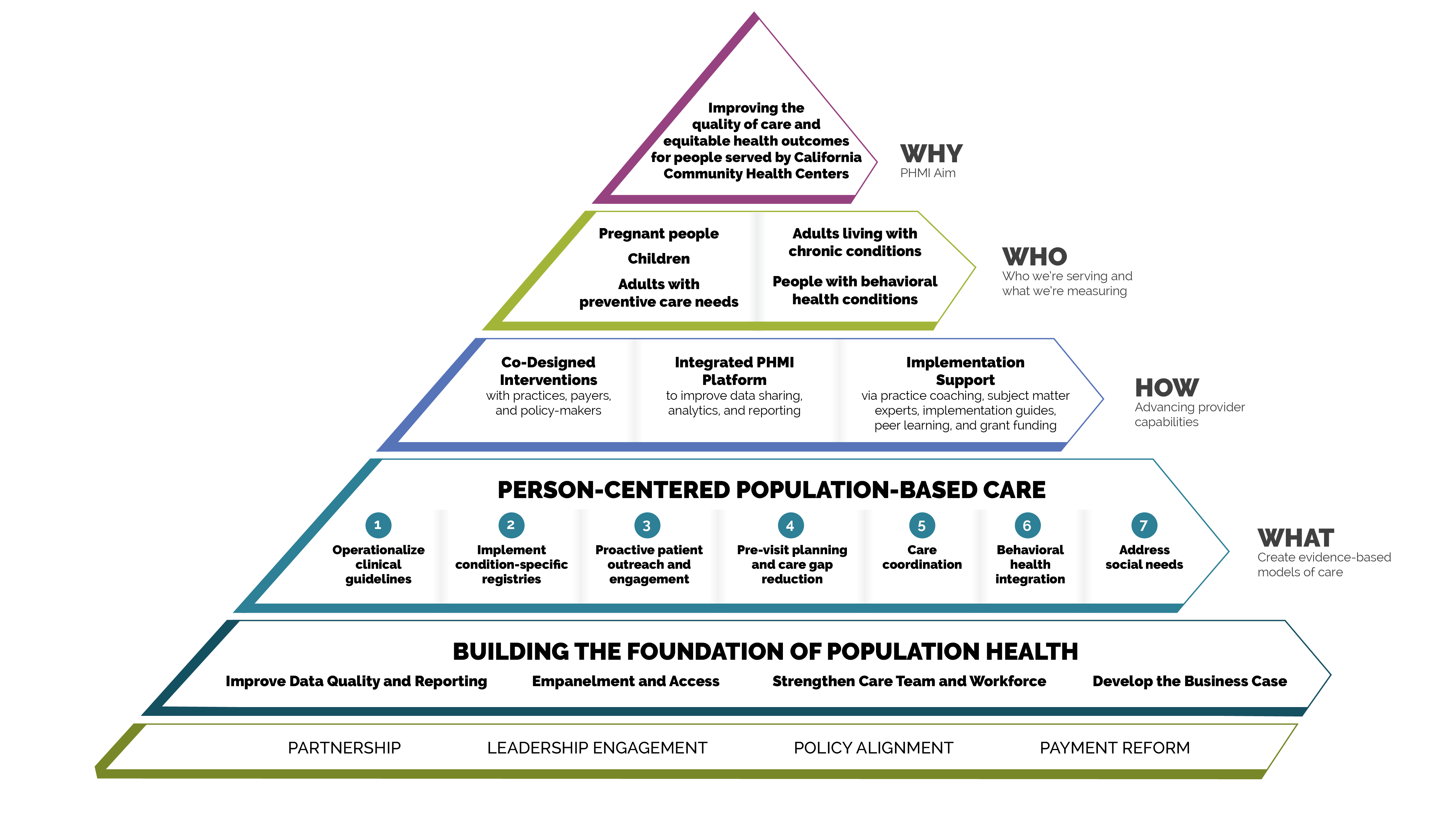
Person-centered population-based care
Each of the key activities advance one or more of the seven person-centered population-based care change concepts:
- Operationalize clinical guidelines.
- Implement condition-specific registries.
- Proactive patient outreach and engagement.
- Pre-visit planning and care gap reduction.
- Care coordination.
- Behavioral health integration.
- Address social needs.
FIGURE 1: PHMI IMPLEMENTATION MODEL
Core and supplemental measures
The measures covered in this guide consist of Healthcare Effective Data and Information Set (HEDIS) measures designated as core and supplemental measures by PHMI. These measures can be considered outcome measures because there is ample evidence that improved timely care will improve overall population health outcomes for prenatal and postpartum care. All measures use standard HEDIS definitions and are aligned with CalAIM and APM 2.0. For information about these measures, reference the PHMI Data Quality and Reporting Guide.
PHMI selected a few core and supplemental measures of focus for this population, though practices can track others that feel important and relevant. This guide provides detailed guidance to improve your practice’s results on the following four core and supplemental measures for pregnant people:
- Prenatal and Postpartum Care (Core Measure).
- Prenatal and Postpartum Care (Timeliness of Prenatal Care) (Supplemental Measure).
- Prenatal Depression Screening and Follow-Up (Supplemental Measure).
- Postpartum Depression Screening and Follow-Up (Supplemental Measure).
Core HEDIS Measures for PHMI
|
PHMI Populations of Focus |
Measures |
|---|---|
Pregnant people |
Prenatal and Postpartum Care Percentage of people with a postpartum visit within seven to 84 days after delivery. |
Supplemental HEDIS Measures for PHMI
|
PHMI Populations of Focus |
Measures |
|---|---|
Pregnant people |
Prenatal and Postpartum Care (Timeliness of Prenatal Care) Percentage of deliveries in which people had a prenatal care visit in the first trimester. |
Prenatal Depression Screening and Follow-Up Percentage of deliveries in which people were screened for clinical depression while pregnant and, if screened positive, received follow-up care. Two rates are reported:
|
|
Postpartum Depression Screening and Follow-Up Percentage of deliveries in which people were screened for clinical depression during the postpartum period and, if screened positive, received follow-up care. Two rates are reported:
|
Measurement strategy and learning system
The core and supplemental measures are part of a larger measurement strategy and learning system, as outlined in Appendix A: Sample, Idealized System Diagram. Key Activity 1: Convene a Multidisciplinary Implementation Team Focused on Pregnant and Postpartum People outlines how your practice can develop a robust measurement system to support this work. In addition to quality assurance and monitoring, measures are also used during practice operations alongside other data for learning to
- Guide the actions of the multidisciplinary implementation team as they use a systematic approach to decreasing inequities and supporting the implementation of key activities across the practice.
- Support the care team’s efforts to advance population health and reduce care gaps through daily, weekly and monthly workflows, as well as continuous identification of opportunities for improvement.
Clinical practice guidelines
The PHMI Clinical Guidelines Advisory Group (CGAG) was established to create a standardized approach to review, adopt and promote established clinical guidelines in the PHMI cohort. For pregnant people, guidance includes prenatal care initiation and prenatal and postpartum depression. For more information, please see the Clinical Practice Guidelines for Key Medi-Cal Populations of Focus.
Figure 2: Clinical guidelines: Prenatal and Postpartum Care (Timeliness of Prenatal Care)
Source |
National Committee for Quality Assurance (NCQA) Healthcare Effectiveness Data and Information Set (HEDIS) |
PHMI measure |
Prenatal and Postpartum Care (Timeliness of Prenatal Care) |
Guideline language |
Ensure a prenatal care visit occurs during the first trimester for pregnant people. |
Definitions |
First trimester: 280 to176 days prior to delivery (or estimated delivery date (EDD)). Prenatal care: Any of the following where the practitioner type is an OB/GYN or other prenatal care practitioner or primary care provider (PCP) meet criteria for a prenatal visit:
|
Figure 3: Clinical guidelines: Prenatal and Postpartum Care (Timeliness of Postpartum Care)
Source |
|
PHMI measure |
Prenatal and Postpartum Care (Timeliness of Postpartum Care) |
Guideline language |
Conduct a postpartum visit in the first three weeks after delivery with a maternal care provider for persons who have delivered a live birth in any setting. After the initial assessment, provide ongoing care as needed, concluding with a comprehensive postpartum visit no later than 12 weeks after birth. |
Definitions |
Postpartum care: Documentation of a postpartum visit to an OB/GYN practitioner, midwife, family practitioner or other PCP. Must include a note indicating the date when a postpartum visit occurred and one of the following:
|
Figure 4: Perinatal Depression Screening and Follow Up (Prenatal)
Guideline Source |
Kaiser Permanente Southern California (December 2022) |
PHMI Measure |
Prenatal Depression Screening and Follow Up (PND-E) |
Guideline Language |
Prenatal Depression Screening (Kaiser Permanente National Guideline Program): Prenatal depression screening is recommended in the first 12 weeks. |
Figure 5: Perinatal Depression Screening and Follow Up (Postpartum)
Guideline Source |
|
PHMI Measure |
Postpartum Depression Screening and Follow Up (PDS-E) |
Guideline Language |
Postpartum Depression Screening (ACOG): Postpartum depression screening is recommended once during the postpartum period. |
Utilizing this guide to improve equitable outcomes
Many key activities in this guide include considerations for utilizing the intervention to improve equitable health outcomes and reduce the effects of racism, bias and discrimination. Key Activity 4: Use a Systematic Approach to Decrease Inequities describes key action steps for how to make an intentional and explicit effort to identify inequities, understand root causes, and reduce those inequities.
This guide also offers resources for going deeper into organizational and ecosystem-level work to advance equitable outcomes through Key Activity 18: Strengthening Community Partnerships and Key Activity 20: Strengthening a Culture of Equity. More information about this approach can be found in the PHMI Equity Framework and Approach.
Integrating behavioral health screening
Integrated behavioral health supports are important for pregnant people, as behavioral health support is likely to boost perinatal health outcomes and enhance patients’ quality of life. One foundational change is to ensure that the care team includes behavioral health staff as core members of the team; this is covered in detail in the Care Teams and Workforce Guide.
We also offer a resource, the Pre-Visit Planning – Gaps in Care Tool, which includes recommended behavioral health screenings.
For pregnant people, foundational key activities include Key Activity 11: Behavioral Health Screening, Including Postpartum Depression. Throughout the key activities in this guide, we have incorporated considerations for providing trauma-informed care and have included a resource for Implementing Population Health Management in Trauma-Informed Ways. For additional information about managing behavioral health conditions beyond screening, please see the Behavioral Health Implementation Guide.
Utilizing this guide to attend to patients’ social needs
For many key activities in this guide, we have highlighted considerations related to social needs at the individual or population level, such as expanding referral networks. A foundational activity is Key Activity 7: Use Social Needs Screening to Inform Patient Treatment Plans, which can help practices better understand and support patient- and population-level needs. Practices can help patients make connections to resources in the community to address issues such as nutrition, childcare, legal and health education needs. For Medi-Cal patients and families with high levels of social need, such as those experiencing homelessness, referrals to Enhanced Care Management and community support programs are available. See Key Activity 19: Provide Care Management for more.
For going deeper in this area, practices can utilize Key Activity 17: Continue to Develop Referral Relationships and Pathways for common social needs and Key Activity 18: Strengthen Community Partnerships to build upon the strengths, infrastructure and resources available in the community. More information about this dual patient- and population- level approach is available in the PHMI Social Health Framework and Approach.
Our theory of change
Our theory of change is that if practices implement the activities contained in this guide, it will lead to improved health and wellbeing outcomes among the pregnant people served by practices. See Appendix B: Theory of Change for a suggested driver diagram.
Foundational Key Activities
Activities that all practices should implement as part of their prenatal and postpartum care protocol.
KEY ACTIVITY #1:
Convene a Multidisciplinary Implementation Team Focused on Pregnant and Postpartum People
This key activity involves all seven elements of person-centered population-based care: operationalize clinical guidelines; implement condition-specific registries; proactive patient outreach and engagement; pre-visit planning and care gap reduction; care coordination; behavioral health integration; address social needs.
Overview
This activity provides guidance for developing, launching and sustaining a multidisciplinary team or task force within your practice who will be responsible for the planning and implementation of all of the foundational key activities in this guide and overseeing related quality improvement and equity efforts as outlined in Appendix A: Sample, Idealized System Diagram.
Why this matters
The implementation team is so important that it appears first in our sequenced list of foundational activities. Improving your practice’s key outcomes for pregnant people and reducing equity gaps requires the aligned efforts of all care teams and nearly all functional areas of the practice, not just those working directly with patients.
Leveraging this intervention to address social needs and equity
This team is responsible for ensuring that all foundational key activities in this guide, including those related to screening for social needs, are implemented. In selecting potential members of this multidisciplinary implementation team, the practice should identify a diverse group of staff who are reflective of the community served and who represent the lived experience of patients. In addition to implementing the key activity focused on applying a systematic approach to decrease health inequities, the team should apply an equity lens to every step outlined in this guide to help ensure that any improvements are equitably spread among the patient population. To achieve optimal functioning and impact, all members of this diverse, multidisciplinary team should have their perspectives proactively included. Be intentional in considering how power structures within your multidisciplinary team (e.g., physicians vs. non-clinical staff or patients) might affect how team members contribute to your care pathways. All voices must have equal weight.
Technology considerations
To enable team coordination, thought must be given to how to access relevant technology, how data capture can be distributed, consistent, and integrated into workflows, and how data is accessible across team members. Where possible, it is desirable to avoid duplication of data entry, siloing of information in stand-alone applications and databases, and the need to work in multiple applications requiring separate logins. Relevant health information technology (HIT) capabilities to support this activity include electronic access to care guidelines, registries, clinical decision support; care dashboards and reports; quality reports; outreach and engagement; and care management and care coordination
See Appendix D: Guidance on Technological Interventions.
Action steps and roles
1. Develop a time-limited group of leaders within the practice to start this process.
Suggested team member(s) responsible: Chief medical officer or equivalent and office manager or quality improvement coordinator.
Start with a small group of leaders from your practice (some of whom will be on the implementation team) who can help refine the charge or scope of work of the implementation team and both identify and engage the people/roles that will be required to implement the scope of work of the team.
2. Develop a preliminary scope of work or charge outlining the responsibilities of the implementation team.
Suggested team member(s) responsible: Time-limited group of practice leaders.
This scope or charge includes but may not be limited to enabling, aligning, leveraging and supporting the planning and implementation of all foundational key activities in this implementation guide for pregnant people so that the practice meets the foundational competencies for providing high-quality prenatal care.
However, there may be further foundation building work needed at your practice in order for you to succeed at the above key activities. The Population Health Management Capabilities Assessment Tool (PhmCAT) is a multidomain assessment that is used to understand current population health management capabilities of primary care practices. This self-administered tool can help your practice identify opportunities and priorities for improvement.
If your practice has not scored highly in the domains of leadership and culture; the business case for population health management, technology and data infrastructure; or empanelment and access, consider implementing the activities listed in the four guides on Building the Foundation before or in parallel to working on key activities related to pregnant people.
3. Identify leadership and key actors for the implementation team.
Suggested team member(s) responsible: Time-limited group of practice leaders.
The multidisciplinary implementation team should include those empowered to make changes in workflows, policies and staff assignments. They should be respected influencers in the organization (early adopters) who can also guide the change management process. They should also include those with expertise in partnering with patients.
- Appoint a “champion” or lead person (e.g., “pregnant people implementation coordinator” to oversee the implementation and coordination of the team.
- Identify key actors who will be the core members of the implementation team. Ensure diversity of position and diversity of gender/race/language. Compensate non-employee members of the team equitably for their time (e.g., patients or community members with lived experience).
- Suggested members of the team focused on pregnant people can include, but may not be limited to:
- A physician clinical leader.
- A nurse clinical leader.
- A community health worker.
- A midwife or advanced practice clinician.
- A comprehensive perinatal health worker (CPHW).
- A social worker or case manager.
- A doula.
- A data lead.
- A mental health provider.
- A representative from a community-based organization or agency who frequently provides social services to your patient population.
- A quality improvement lead.
- Community members most represented in the group with the poorest outcome.
- Invite identified people to become part of the implementation team and ensure that they have designated time for their participation and/or are compensated equitably for their time.
Teams should engage representation from information technology (IT) to support the work of pulling data from the electronic health record (EHR) and embedding updated data into tracking and evaluation.
4. Launch the implementation team and set it up for success.
Suggested team member(s) responsible: Clinical coordinator, chief operating officer (COO), or chief marketing officer (CMO).
This work includes:
- Ensuring that the team understands their charge or scope of work.
- Developing a team charter outlining this work.
- Defining roles and responsibilities including the anticipated commitment (in hours) on a monthly basis. Create a compensation plan for nonemployee members of your team (e.g., patients or community members).
- Establishing a meeting structure, file structure and communications structure to support effective, efficient work.
- Dedicating time and effort to forming, storming, norming and performing as a team. The Resource: Team Communication and Working Styles Template is one tool that team members can complete and share with other teammates to accelerate this process.
- Understanding baseline data related to outcomes of interest (e.g., timely postpartum visits and baseline prenatal depression screening), along with data related to known and perceived barriers to these outcomes. Assess stratified outcomes data to identify quality performance disparities in particular subpopulations.
- Prioritizing elements within the scope of work, informed by baseline data and identified population needs
5. Develop a simple yet robust measurement strategy and learning system to guide your improvement efforts.
Suggested team member(s) responsible: QI lead or equivalent.
A learning system enables a group of people to come together to share and learn about a particular topic, to build knowledge and speed up improved outcomes. A simple yet robust measurement strategy and learning system:
- Contains a balanced set of measures looking at outcomes, processes and possibly unintended secondary effects (e.g., increased cycle time and impact on team well-being).
- Incorporates the patient perspective and the perspective of staff (front desk and others), care team members, and management.
- Allows the team to determine if the process or system has improved, stayed the same, or gotten worse.
- Helps guide improvement efforts and informs practice operations. See Appendix A: Sample, Idealized System Diagram for a sample system diagram for how your measurement strategy can be used to support practice operations.
Your practice should track the core and supplemental measures for prenatal and postpartum care: timeliness of prenatal and postpartum care; prenatal depression screening and follow-up; and postpartum depression screening and follow-up. These can be considered outcome measures because there is ample evidence that earlier entry into care, and regular monitoring for depression will improve overall population health outcomes for pregnant people.
In addition to the core and supplemental measures, practices should track process measures and balancing measures. Appendix C: Developing a Robust Measurement Strategy describes and defines the key milestones in the development of a robust measurement strategy, including definitions for each of these terms.
Suggested process measures:
- The number of patients who have an appointment scheduled for a postpartum visit prior to facility discharge after birth.
- Percentage of adults who are sent a reminder regarding postpartum visit who attend the visit.
Suggested balancing measures:
- One or more measures related to patient satisfaction.
- One or more measures related to staff satisfaction.
- One or more measures related to appointment availability (wait times).
Practices can also look at other metrics to understand the progress of specific improvement initiatives over time. These may include:
- Progress on the Population Health Management Capabilities Assessment Tool (PhmCAT).
- Progress towards foundational competencies listed in this implementation guide. For example, “Yes or No: Did your practice achieve the following foundational competency ‘Develop a process for screening pregnant and postpartum people for depression, using evidence-based tools’?”
- Any other care gaps, clinical guidelines or measures your practice feels are important to prioritize.
Applying an equity lens
Your practice is likely achieving better outcomes with some patients than others. To understand who the practice is achieving poorer adult prevention outcomes for, practices should stratify their data based on race, ethnicity and language (REAL); sexual orientation and gender identity (SOGI); and other patient characteristics (e.g., social needs, etc.). See more in Key Activity 4: Use a Systematic Approach to Decreasing Inequities Within the Population of Focus. The ability to segment data in such a manner can lead to profound insights about structural challenges driving some of the health outcomes. The Advancing Equity Through Data Quality and Reporting section of the PHMI Data Quality and Reporting Guide provides more guidance on this.
Putting it all together
We recommend that your practice keep your measurement strategy in a single spreadsheet. The Measurement Strategy Tracker contains all the fields we believe are most useful and can be customized by your practice to meet your needs.
6. Plan and implement regularly scheduled meetings of the implementation team.
Suggested team member(s) responsible: QI lead or equivalent.
- Hold time on team members' calendars for standing meetings. Consider biweekly (twice monthly) meetings to start with. The frequency, duration and focus of these meetings may change as you consider additional populations or subpopulations, additional sites or locations, and the changing nature of the work.
- Develop a system to efficiently report on all work streams and track follow-up items. The Action Plan Template is one tool that can be used to focus your team around the foundational competencies and define responsibility for actions steps to be taken for each project your team has prioritized to work on.
7. Make adjustments based on data from the team’s measurement strategy and feedback loops.
Suggested team member(s) responsible: Multidisciplinary team.
- Review data and feedback at least monthly and adapt efforts as needed. Adaptation could include any or all of the following:
- Amending the charge or scope of work.
- Modifying meetings or meeting structures.
- Changing the team composition (adding or removing members).
- Gathering feedback from patients and practice staff to modify the changes implemented.
- Refining key activities to better meet the needs of patients and practice staff and to improve outcomes or reduce inequities.
- Modifying the measurement strategy and/or feedback loops to better understand what is and isn’t happening.
- On an annual basis, the team’s charter and core membership should be reviewed. As the implementation team's goals are met, the team could disband, meet less frequently (e.g., twice per year), or fold this meeting into a similar standing meeting that occurs separately.
Evidence base for this activity
Pandhi N, Kraft S, Berkson S, Davis S, Kamnetz S, Koslov S, Trowbridge E, Caplan W. Developing primary care teams prepared to improve quality: a mixed-methods evaluation and lessons learned from implementing a microsystems approach. BMC Health Serv Res. 2018 Nov 9;18(1):847. doi: 10.1186/s12913-018-3650-4. PMID: 30413205; PMCID: PMC6230270.
KEY ACTIVITY #2:
Review Perinatal Care Clinical Guidelines Including Specialty Referral
This key activity involves the following elements of person-centered population-based care: operationalize clinical guidelines.
Overview
Clinical care guidelines for pregnant people are evidence-based recommendations that help healthcare providers and pregnant people make informed decisions about the optimal care during pregnancy and childbirth. For example, both PHMI Clinical Practice Advisory Group Guidelines and the American College of Obstetricians and Gynecologists (ACOG) recommend as a clinical care guideline that a first prenatal care visit occur during the first trimester of pregnancy. Clinical care guidelines should be incorporated into systems to aid practitioners in providing the most effective evidence-based recommendations and treatments to patients. Clinical care guidelines have been shown to reduce patient harm by enhancing communication and standardization. In medical institutions, the application of protocols and guidelines is frequently delayed due to a lack of healthcare provider awareness or overly complex clinical algorithms. However, it has been demonstrated conclusively that using clinical care guidelines such as protocols and checklists improves outcomes, and their use is strongly encouraged. At the patient level, clinical guidelines can be applied to create a flag or alert in the EHR to notify the care team of gaps in obstetric and preventive services. These alerts enable the care team to efficiently identify necessary services related to patient visits.
Why this matters
Every year, over four million people give birth in the United States, with one million experiencing one or more complications during pregnancy, labor and delivery or the postpartum period.[5] According to studies, up to 60% of all pregnancy-related deaths may be prevented if people had better access to healthcare, received better quality care, and modified their health and lifestyle behaviors.[6] Timely and appropriate prenatal and postpartum care can provide the groundwork for new parents’ and infants' long-term health and well-being.[7] Clinical guidelines are one component of improving the quality of perinatal care.
Leveraging this intervention to improve equitable health outcomes
Clinical guidelines can help address equity in perinatal outcomes by providing guidance on how to identify and address disparities in care. For example, guidelines may recommend that healthcare providers screen patients for social needs, such as transportation, food access, economic insecurity, education and housing, which can impact maternal health outcomes. Guidelines may also recommend that healthcare providers use evidence-based practices that have been shown to improve outcomes for all patients, regardless of race or ethnicity. By following clinical guidelines, healthcare providers can ensure that they are providing evidence-based, equitable care to all patients.
Leveraging this intervention to attend to patients’ social needs
Leveraging the adoption of perinatal clinical guidelines can help patients and families by providing systems to assess potential social needs and thus provide patients with more comprehensive, respectful, and culturally appropriate care. For example, the National Institute for Health and Care Excellence (NICE) guideline on pregnancy and complex social factors recommends providing training on how to communicate effectively and sensitively with pregnant people who face multiple disadvantages.[8]
Technology Considerations
Prenatal care visits are highly structured and can therefore be supported through the use of highly structured visit templates in the EHR. Engagement of the care team can be supported through specialized applications such as care coordination and population health management applications, and/or through the creation of freestanding databases. Relevant HIT capabilities to support this activity include: electronic access to prenatal care guidelines, registries, clinical decision support, care dashboards and reports, quality reports, outreach and engagement, and care management and care coordination.
See Appendix D: Guidance on Technological Interventions.
Reports should have the capacity to filter by provider, location and care team, where applicable.
Access to outside data may be a consideration or requirement (e.g., California Immunization Registry (CAIR) or immunization registry data, referral consultation reports, hospitalization data, and data from other practices) as services received outside the health center may be part of compliance. While claims data may be helpful in this regard, lag time may impact its usefulness. Patient-facing applications should be strongly considered to assure patients are informed and appreciative of the nature and importance of recommended care.
Action steps and roles
Please see the Clinical Guidelines for Prenatal Care in the introduction for the PHMI Clinical Practice Guidelines for Key Medi-Cal Populations of Focus.
In addition, the American College of Obstetricians and Gynecologists (ACOG) recommends early postpartum follow-up care, including screening for depression and anxiety, for all postpartum patients.
1. Assess the needs and priorities of the organization and its stakeholders, such as patients, providers, managers, and policymakers.
Suggested team member(s) responsible: Medical director or their designee.
Identify organizational capacity to review and implement or update current clinical care guidelines. Assess organizational priorities as well as patient and provider priorities, and determine points of alignment or potential conflict.
2. Identify the gaps and barriers in the current practice and where clinical care guidelines could help improve outcomes.
Suggested team member(s) responsible: Medical director or their designee.
Review perinatal clinical care guidelines currently used in clinical care. Evaluate if these guidelines cover the range of best practices or if new care guidelines need to be implemented.
3. Review relevant and reliable clinical care guidelines that are based on the best available evidence and aligned with the organization’s goals and values.
Suggested team member(s) responsible: Medical director or their designee.
Review Clinical Guidelines Advisory Group (CGAG) recommendations on timeliness of prenatal and postpartum care. Determine additional sources to review for additional perinatal care guidelines. See the resources at the end of this activity for further information on evidence-based clinical care guidelines.
4. Consider the local context, resources and preferences of the organization and its stakeholders. Integrate the guidelines to suit the specific needs and circumstances of the organization.
Suggested team member(s) responsible: Medical director or their designee, patients, clinical team.
Care guidelines reflect recommendations for best practices. To best implement these guidelines into clinical practice, careful consideration should be taken around how they intersect with the organization's unique needs.
5. Monitor and evaluate the process and outcomes of guideline implementation using appropriate indicators and methods.
Suggested team member(s) responsible: Medical director or their designee, QI team, clinic managers.
Utilize care gap reports (Key Activity 3: Use Care Gap Reports or Registries to Identify All Patients Eligible and Due for Care) and other metrics to evaluate whether implementation of the guidelines are improving desired metrics, such as access to prenatal care in the first trimester or screening for perinatal depression.
6. Collect data on the adherence to the guidelines, the quality and safety of care, the patient satisfaction and outcomes, and the costs and benefits of implementation.
Suggested team member(s) responsible: Medical director or their designee; QI team, clinical team.
Construct mechanisms to evaluate guideline implementation from multiple perspectives: clinician, patient, QI team.
7. Analyze data to identify problems, challenges, successes and lessons learned. Make modifications to care guideline implementation as needed.
Suggested team member(s) responsible: Medical director or their designee; QI team, clinical team.
Based on collected data, assess for patterns of workarounds, inadequate implementation, workflow challenges, and patient concerns. Identify successes to inform future implementation strategies.
8. Provide feedback and support to the stakeholders involved in guideline implementation.
Suggested team member(s) responsible: Medical director or their designee, clinic manager, clinical staff.
Convey information from action item #6 to relevant team members. Encourage ongoing communication regarding implementation of care guidelines.
9. Sustain and scale up guideline implementation by ensuring ongoing commitment, engagement and support from the organization’s leadership and stakeholders.
Suggested team member(s) responsible: Medical director or their designee.
10. Share best practices and experiences with other healthcare organizations that are interested in adopting or implementing clinical care guidelines.
Suggested team member(s) responsible: Medical director or their designee.
Resources
KEY ACTIVITY #3:
Use Care Gap Reports or Registries to Identify All Patients Eligible and Due for Care
This key activity involves the following elements of person-centered population-based care: implement condition-specific registries; address social needs.
Overview
This foundational activity provides detailed guidance on how to reliably and efficiently develop and use a regularly updated list of all pregnant patients eligible for recommended care through a care gap report or registry. Like registries used to identify patients who require preventive services for chronic diseases, a perinatal care registry can be used to track all perinatal care patients and assist in ensuring their individual prenatal and postnatal care needs are addressed in a timely manner. The registry should be integrated with the practice’s EHR or population health tool. It should include a list of all perinatal care patients by week of gestation, their corresponding perinatal-specific and general preventive care gaps (either due or overdue), and pregnancy risk level. The care team utilizes the perinatal care registry to monitor the completion of necessary services throughout the episode of pregnancy.
Care gaps are gaps between the recommended care that a patient should receive according to clinical guidelines and protocols and the care a patient has actually received. Most EHRs already have a module that identifies what services are due for each patient. Care gap reports or registries are recommended as a way to monitor the perinatal care population to ensure that pregnant patients receive timely, comprehensive perinatal care.
FIGURE 4: EXAMPLE CARE GAP REPORT FOR AN INDIVIDUAL PATIENT
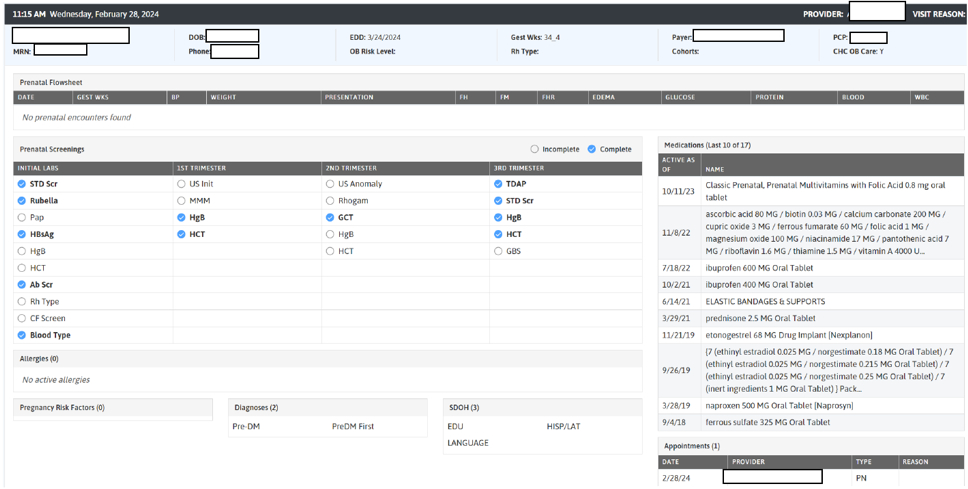
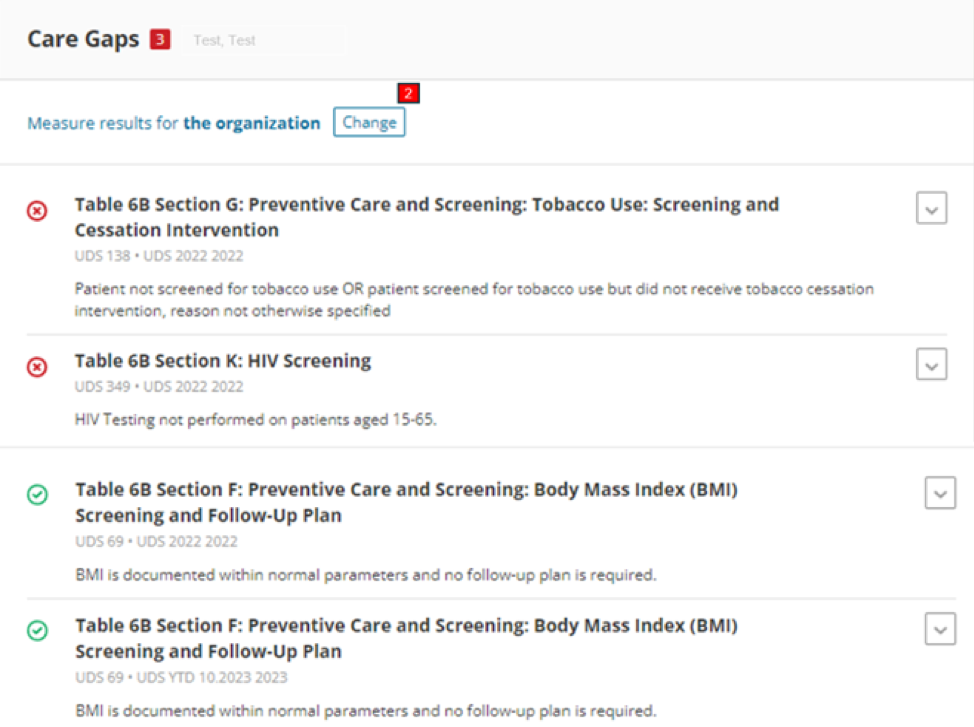

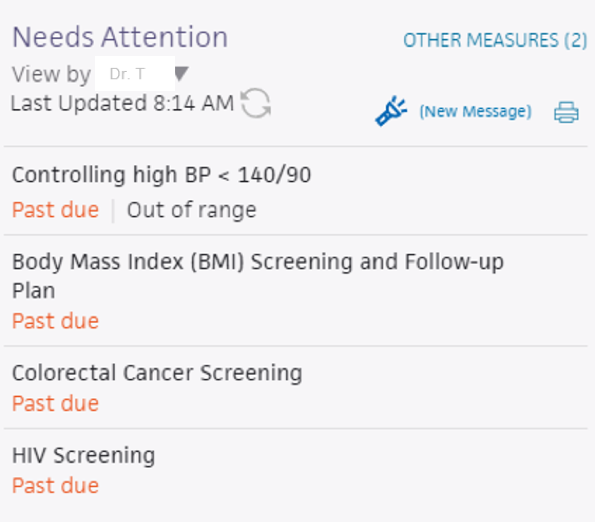
FIGURE 5: EXAMPLE OF A CARE GAP REPORT FOR A PANEL OF PATIENTS
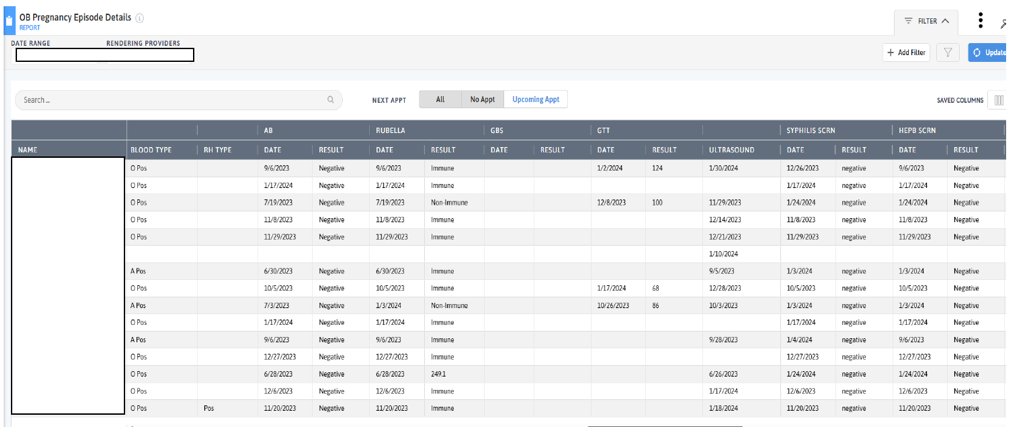
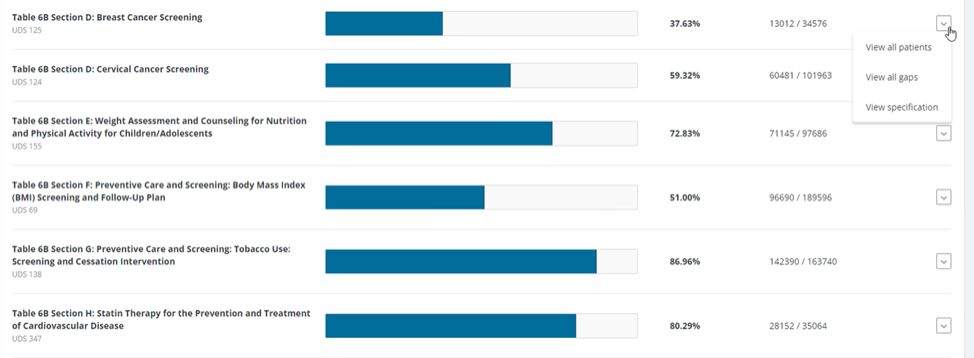
FIGURE 6: EXAMPLE OF A PRENATAL CARE GAP REPORT AT THE POPULATION LEVEL

Rather than put the responsibility of searching through charts or remembering which patients need further preventive care or follow-up on the individual care team member, this key activity demonstrates how the practice can efficiently leverage EHRs for all its patients.
Why this matters
Care gap reports are essential in understanding how well practices are meeting clinical care guidelines for various measures. This awareness supports improvement, consistency and reliability in meeting care guidelines. At the care team level, gap reports focus on due or overdue labs, screenings, or other interventions for patients assigned to your care team. These lists can be used to:
- Support improvements to the pre-visit planning process, develop standing orders, and improve other routine clinical workflows designed to systematically identify and address gaps in care.
- Remind providers of needed orders for a clinical visit.
- Prioritize patients for whom care teams should provide proactive outreach and reminders for engaging in care.
- Support quality improvement efforts with an equity lens.
Actively identifying and acting on care gaps ensures all patients assigned to your practice receive timely care. This approach reduces missed or delayed diagnoses; for example, supporting patients completing gestational diabetes (GDM) screening during the recommended interval avoids delays in GDM treatment. At a systems level, this reduces the burden on the healthcare system by preventing more severe health issues in the future.
For pregnant people, care gap reports can identify patients who are due for regular or infrequently required screenings in accordance with clinical care guidelines, including guidelines that may be established by specific payors. Cervical cancer screening and immunization needs are some examples. Other preventive and maintenance services are noted in the resource Pre-Visit Planning – Gaps in Care Tool.
Leveraging this intervention to improve equitable health outcomes and address social needs
Many patients experience barriers in accessing care due to structural and individual racism, homophobia, xenophobia, and other biases that deny historically disadvantaged individuals and groups from receiving equitable services. Defining clear criteria and gaps for patients due for specific screenings or preventive services helps to illuminate groups who have not had equitable access. It also combats biases by standardizing expectations for what constitutes quality standards of care for all clients.
Staff can identify potential barriers for patients by using enhanced care gap reports to filter and display the data alongside demographic information, social needs, behavioral health needs, and communication preferences. This information can be used to promote a person-centered approach when designing the care plan, such as conducting visits and outreach in the patients’ preferred language.
Furthermore, care gap reports that segment data into cohorts based on demographic and other personal information may help the team identify disparities in care, access and outcomes, which can inform improvement efforts. Care gap reports can be used during pre-visit planning to identify people for whom social needs screening has not yet been completed. See Key Activity 6: Develop of Refine and Implement a Pre-Visit Planning Process for more information. This creates an opportunity to identify unmet social health needs and connect patients with relevant resources.
Technology Considerations
Many EHRs already have a module that identifies what services are due for each patient, while others do not. Where this functionality is available, it may not be configurable to align with the health center’s specific protocol or they may not be able to incorporate outside data. Other options for developing registries include supplemental applications, population health platforms and freestanding customized databases that draw data from the EHR and other sources.
A registry can be thought of as simply a list of patients sharing specific characteristics that can be used for tracking and management. Both care gap reports and registries should have the capacity to segment patients by relevant variables that indicate the need for specialized care elements or risk factors.
Care gap reports may be embedded in electronic health records or made available through other technology channels (see Appendix D: Guidance on Technological Interventions) and are useful both at the individual patient level and aggregated to identify groups of patients to facilitate population-level management through registries.
Other relevant HIT capabilities to support and relate to this activity include: prenatal care guidelines, care dashboards and reports, quality reports, outreach and engagement, and care management and care coordination.
See Appendix D: Guidance on Technological Interventions.
Access to outside data may be a consideration or requirement (e.g., CAIR or immunization registry data and data from other practices) as services received outside the health center may be part of compliance. While claims data may be helpful in this regard, lag time may impact its usefulness. Patient-facing applications should be strongly considered to ensure they are informed and appreciative of the nature and importance of recommended care. In California, many healthcare organizations are required or have chosen to participate in the California Data Exchange Framework (DxF), which can facilitate data sharing between clinics, managed care plans (MCPs) and other partners.
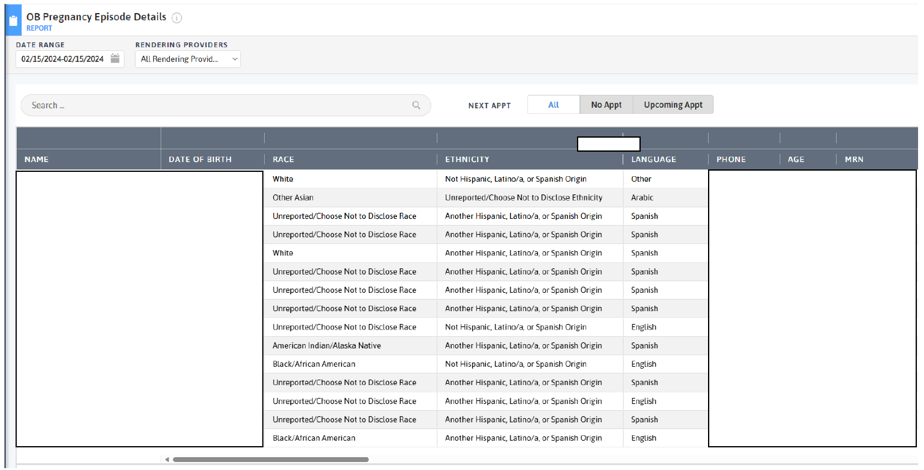
FIGURE 7: REGISTRY OF PRENATAL PATIENTS INCLUDING REAL DATA AND PHONE NUMBER
Action steps and roles
1. Plan the care gap report.
Suggested team member(s) responsible: Site director and panel manager or data analyst. If it is not clear how the report can be produced, this step may involve one or more people from the practice will work on the EHR and, possibly, the EHR vendor.
As a team, decide what screenings or treatment guidelines are appropriate for your population of focus and prioritize the most important care gaps to run reports on. Start with the core and supplemental measures and any process measures your practice is tracking, and consider if there are any other gaps, clinical guidelines, or measures your practice feels important to prioritize.
Identify the inclusion criteria for each report, such as age, any exclusion criteria, and factors that make someone high risk.
Important resources:
- U.S. Preventive Services Task Force (USPSTF) recommended preventive services for the maternity population.
- ACOG’s Optimizing Postpartum Care.
- Postpartum parental depression screening registries, prenatal labs and education checkpoints, such as outlined in the Comprehensive Perinatal Services Program (CPSP).
2. Build the report.
Suggested team member(s) responsible: Data analyst.
Determine whether the EHR has an existing report or one that can be modified to fit the inclusion criteria. You should talk to staff who are familiar with the electronic record. In some cases, it may be necessary to consult with the EHR vendor to confirm this information and how to run the report.
Leveraging technology for automation: Each EHR is different, but they generally offer guidance or support on developing care gap reports. In the absence of automatic reports, it may be necessary to engage other staff with the capacity to use other reporting software to develop reports from EHR data.
The care gap format should include:
- Criteria for inclusion in the report.
- The overall compliance rate for the care gap being measured.
- All patients eligible for the screening and their addresses and phone numbers.
- The last date the test was performed, if known or if applicable, the previous results, and the type of test used.
- Preferred method of communication (e.g., phone, email, text).
Reports should be able to display and/or disaggregate the data based on:
- Race, ethnicity and language (REAL) as well as sexual orientation and gender identity (SOGI).
- Any known social or behavioral needs.
- Communication preferences or other preferences that would inform the screening modalities offered, such as documented refusal of prior screenings.
- Data on any other characteristic, including insurance data, that could pose a barrier to completing screening.
3. Standardize the data format.
Suggested team member(s) responsible: Panel manager or data analyst.
Standardizing the data format and where it is entered is critical to ensuring accuracy in the resultant report. Once you know that a report can be produced, understand the specific data elements that are needed to produce the reports.
Document how each data element must be entered into the EHR in order to populate the fields needed for reporting. In some cases, data on completion of screening must be entered by hand (e.g., when the test is performed by a lab that does not communicate with the legacy EHR). Doing this will require a decision on the part of the practice as a whole and may require staff training and reinforcement on an ongoing basis. Where issues or apparent confusion are identified, regular discussion at team huddles or staff meetings will help in maintaining a standard approach.
Tip: Assign responsibility for the initial review of the reports to confirm data integrity.
4. Develop workflows to support improved patient screening and preventive care completion rates.
Suggested team member(s) responsible: Panel manager and care team.
Identify staff members responsible for the ongoing running and review of care gap reports. Formalize workflow to integrate care gap data into daily clinical practice. Determine who has access to these reports (medical assistants, providers, care coordinators, etc.).
At the patient level, ensure that the care gap report can be used for or linked with reminders or alerts for clinicians, as well as for sending reminders to patients who need to come into the practice for recommended pregnancy-related care or testing.
Depending on communication preferences that have been expressed by patients, the patient care gap report may be exported to an automated reminder system that can trigger reminders by phone, text, email, or postal mail.
In addition, as part of the practice’s pre-planning process, patient care gaps should be reviewed and flagged as part of the daily huddle. See Key Activity 6: Develop or Refine and Implement a Pre-Visit Planning Process for more details.
5. Develop a process for review of gaps at the population level.
Suggested team member(s) responsible: Panel manager.
Set a report frequency to review care gap reports at regular care team meetings or huddles in order to develop a plan for improvement at the population level. This may include an outreach campaign to build community awareness of the importance of prenatal and postpartum care and the availability of easily accessed, affordable prenatal and postpartum services.
One limitation of care gap reports for the perinatal population is that they typically only identify patients who have presented to receive care and received confirmation of pregnancy. Patients who have received a positive pregnancy test result within emergency departments, urgent care, or freestanding family planning clinics will not show up within an organization’s care gap report for timely prenatal care. Due to the sensitivity of pregnancy-related services, when considering population-level concerns, patient confidentiality is paramount.
6. Monitor the care gap report for accuracy and completeness.
Suggested team member(s) responsible: Panel manager or data analyst.
It is critical to have bidirectional feedback with the practice’s care team about any real or potential errors in the care gap report, such as:
- Errors in how the data is entered compared to what is required under the new standardized data format.
- Patients who are eligible for and due for screening who are missing from the report.
- Patients who have recently been screened who are still listed as due for a screening.
Errors should be investigated through a chart review. If errors in the report specifications are discovered, the care gap report or process for producing the report should be modified. If the issue is incorrect documentation, staff training and reinforcement of documentation standards will be required.
Additional consideration for sustainability: Ensure there is an internal process for updating the criteria included in the EHR for care gap reports as clinical guidelines change.
KEY ACTIVITY #4:
Use a Systematic Approach to Decrease Inequities within the Population of Focus
This key activity involves all seven elements of person-centered population-based care: operationalize clinical guidelines; implement condition-specific registries; proactive patient outreach and engagement; pre-visit planning and care gap reduction; care coordination; behavioral health integration; address social needs.
Overview
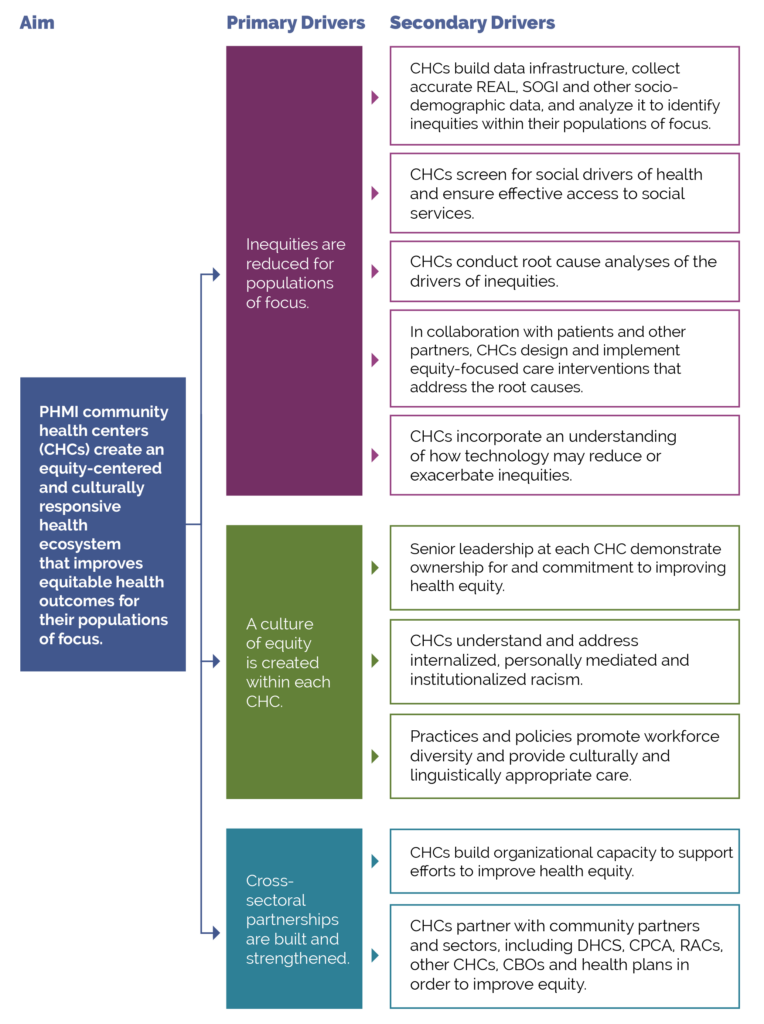
This activity provides guidance for a systematic, evidence-based approach for identifying and then reducing inequities for pregnant people. It focuses on the first primary driver in PHMI’s Equity Approach: Reduce inequities for populations of focus.
FIGURE 8: PHMI EQUITY DRIVER DIAGRAM
Why this matters
Black women have the highest rates of maternal mortality in the United States – three times higher than white women. These inequities are often a direct result of racism, particularly institutionalized racism, which is the differential access to the goods, services and opportunities of a society by race.[9] Limited access to quality healthcare, provider implicit bias and social determinants of health all also contribute to disparate maternal mortality rates. Improving your practice’s key outcomes for pregnant patients requires a systematic approach to identifying equity gaps (e.g., who your practice is not yet achieving equitable outcomes for) and then using quality improvement (QI), collaborative design, systems thinking and related methods to reduce these equity gaps.[10]
Inequitable outcomes are generally most acute among persons of color, immigrants, persons speaking a preferred language other than English, and other populations that have been marginalized. As we work to eliminate inequitable health outcomes, we need to understand factors that contribute to these inequities.
Part of this work includes recognizing that race is a social construct determined by society’s perception. Racial health inequities are evidence that the social categories of race and ethnicity have biological consequences due to the impact of racism and social inequality on people’s health[11]. It is also critical to recognize that we have policies, systems and procedures that unintentionally cause inequitable outcomes for racial, ethnic, language and other minorities, in spite of our genuine intentions to provide equitable care and produce equitable health outcomes.
Technology Considerations
Accessing accurate data to identify and monitor inequities is fundamental to the key actions outlined below.
See Appendix D: Guidance on Technological Interventions.
EHRs can capture basic REAL, socioeconomic, SOGI and social needs-related data but may, in some cases, lack granularity or nuances that may be important to identifying key subpopulations. Mismatches between how the Uniform Data System (UDS) captures REAL data versus how EHRs capture or MCPs report data can also create challenges. This may require using workarounds or modifying your EHR to capture these details. You will also have to align other data systems or applications that are collecting demographic information in alignment with your needs. Furthermore, tracking inequities in accessing services not provided by the health center may also require attention data sources or applications outside the EHR.
Health centers should also be alert to the potential for technology as a contributor to inequities. For example, patient access to telehealth services from your practice may be limited by the inequitable distribution of broadband networks and patient financial resources (e.g., I phones, tablets and cellular data plans). EHR-embedded algorithms used to stratify populations by risk may also contain inherent racial biases. The Techquity framework can be a useful way to structure an approach to assure that technology promotes rather than exacerbates disparity.
Language, literacy levels, technology access and technology literacy should also be considered and assessed against the populations served at the health center.
Finally, attention needs to be paid to the use of best practices in collecting the data, accurate categories in the technologies in which it is collected and stored, and adequate training and monitoring of staff responsible in order to assure reports and analysis have a valid basis.
Relevant HIT capabilities to support this activity include: care guidelines, registries, clinical decision support (modifications required to consider disparate groups), care dashboards and reports, quality reports, outreach and engagement, and care management and care coordination.
Action steps and roles
1. Build the data infrastructure needed to accurately collect REAL, SOGI, social needs and other demographic data.
Suggested team member(s) responsible: Data analyst.
- Race, ethnicity and language (REAL).
- Sexual orientation and gender identity (SOGI).
The PHMI Data Quality and Reporting Guide provides guidance and several resources for collecting this information. According to this guide, the initial step in addressing disparities is to collect high-quality data that fosters a holistic view of patient characteristics and needs. This entails incorporating REAL data, demographic data (age, SOGI, geography) and social needs data. By collecting and monitoring this information, healthcare practices can gain valuable insights into disparities in access, continuity and health outcomes. Steps two to four below provide more information on this process.
Collecting REAL information allows for practices to identify and measure disparities in care while also ensuring that practices are able to interact successfully with patients. This is done by understanding patients’ unique culture and language preferences.[12] KHA Quality has a toolbox that assists with REAL data collection.
The Uniform Data System (UDS) Health Center Data Reporting Guidance (2023 Manual) provides detailed guidance on REAL and SOGI. While UDS does not currently require that practices report on the preferred language of each patient, practices should make an effort to identify and record each patient’s preferred language due to UDS reporting still requiring for languages other than English to be reported.
Accurate data collection requires appropriate fields and options in the EHR and other employed technologies, as well as appropriate human workflows in collecting the data. Staff responsible for data collection should be continuously trained and assessed for best practices in data collection, including promotion of patient self-report.
In addition, practices should work to ensure that patients understand the importance and use of this information to help them feel comfortable and support its collection. High rates of “undetermined” or “declined” responses in these fields may be indicative of the need to attend to these staff training needs.
Collecting this data is important, especially to obtain a complete picture of health for patients who identify as transgender or gender-expansive. Perinatal services are typically highly gendered and by understanding the needs of patients more fully, Providers can make more informed decisions for the best treatment of their patients. World Professional Association for Transgender Health (WPATH) has provided further guidance regarding standards of care related to gender diversity.
2. Use the practice’s electronic health record (EHR) and/or population health management tool to understand inequitable health outcomes at your practice by stratifying your data.
Suggested team member(s) responsible: Data analyst.
This includes reviewing your care gap report or care registry and being able to stratify all of the following:
- Core measures for the population of focus.
- Supplemental measures for the population of focus.
- Process measures for the population of focus.
Stratify this data by:
- Race, ethnicity and language (REAL).
- Sexual orientation and gender identity (SOGI).
- Other factors that can help identify subpopulations in need of focused intervention to reduce an equity gap (e.g., immigrants, people experiencing homelessness, etc.).
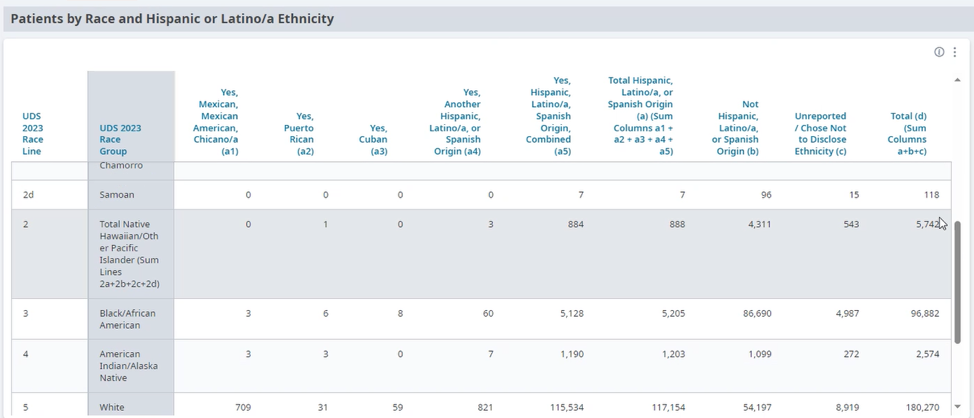
FIGURE 9: EXAMPLE OF DATA STRATIFIED BY RACE AND ETHNICITY
This is not a one-time event, but rather a continuous process (see step 13 below) and should be done in tandem with step three below.
Each practice should define the frequency of review and use of their registry to stratify data. In early use, the stratified data will support the identification of areas of inequity and allow interventions to be prioritized.
3. Screen patients for social needs.
Suggested team member(s) responsible: Care team.
The Key Activity 7: Use Social Needs Screening to Inform Patient Treatment Plans provides guidance on screening patients for health-related social needs and how the information can begin to be used to inform patient treatment plans, including referral to community-based services.
This is not a one-time event, but rather a continuous process and should be done in tandem with step two above.
4. Analyze the stratified data from steps two and three to identify patterns in inequitable outcomes within the population of focus.
Suggested team member(s) responsible: Data analyst, QI leads, care team.
This includes:
- Using data tools to visualize and understand disparities across different populations or subpopulations.
- Data over time (using run charts).
- Exploring trends, patterns and significant differences to understand which demographic groups will require a focused effort to close equity gaps.
This is not a one-time event, but rather a continuous process (see step 13 below) and should be done in tandem with step two (above) and step four (below).
Periodic review of the stratified data allows for the recognition of gap closures and the emergence of new disparities.
5. Use a root cause analysis to identify improvement approaches for subpopulations with lagging health outcomes.
Suggested team member(s) responsible: Multidisciplinary team.
Select root cause analysis approaches that work best for the equity gap you are closing:
- Engage and gather information from patients affected by the health outcome in your root cause analysis (see step six).
- Brainstorming.
- Systems thinking (understanding how interconnected social, economic, cultural and healthcare access factors may be impacting the health outcome).
- Tools that rank root causes by their impact and the feasibility of addressing them (e.g., prioritization matrix and/or an impact effort matrix)
- Visual mapping of root causes and effects (e.g., fishbone diagram).
- Perform focused investigations into selected root causes and gather qualitative data through interviews, surveys or focus groups with the subpopulation of focus.
Present the findings to a broader group of stakeholders to validate the identified root causes and gain additional insights. Incorporate their feedback and refine the analysis, as needed.
6. Partner with patients to build successful strategies addressing inequitable outcomes.
Suggested team member(s) responsible: Care team and people with lived experience (patients who are members of the population(s) of focus).
Using one or more human-centered design methods, such as focus groups, Journey Mapping, etc. (see links to these methods below), engage patients to better understand perspectives that may influence the health outcome of interest. This may include collecting information on:
- Values, needs and preferences.
- Experiences with outpatient prenatal care, intrapartum care at partnering hospital(s), and both inpatient and outpatient postpartum care.
- Cultural beliefs, including traditional healing practices.
- Level of trust in healthcare generally and in the topic of focus specifically (e.g., access to prenatal care visits, experience of perinatal depression screening, etc.).
- Barriers to accessing care.
- Barriers to remaining engaged in care.
- Trusted sources of information or communication mechanisms.
- Their ideas for improving health outcomes.
The patients you partner with for this and other steps in this key activity may be part of a formal or informal patient group and/or identified and engaged specifically for this equity work. Fairly compensating patients for participating in improvement activities is a best practice.
Selected resources on human-centered design and collaborative design:
- Center for Care Innovations (CCI) Human Centered Design Curriculum via CCI Academy.
- IDEO’s Field Guide to Human-Centered Design.
- IDEO’s Design Kit: Methods.
7. Identify key activities in this guide that address or partially address the root causes of the identified equity gaps.
Suggested team member(s) responsible: Care team and people with lived experiences.
Based upon the insights your practice has developed for a population of focus and your root cause analysis, determine which of the key activities could address or partially address the equity gap.
Most of the key activities either explicitly address an equity challenge or can be adapted to better address an equity challenge. Examples of key activities that can be adapted to reduce identified equity gaps include but are not limited to:
- Key Activity 12: Proactively Reach Out to Patients Due for Care.
- Key Activity 7: Use Social Needs Screening to Inform Patient Treatment Plans (such as providing a referral for one of the CalAIM Community Supports).
- Key Activity 13: Coordinate Care.
- Key Activity 18: Strengthen Community Partnerships.
8. Develop new strategies and ideas to address the identified equity gaps.
Suggested team member(s) responsible: Care team and people with lived experience.
If one or more of your root causes cannot be addressed fully through key activities, use one or more human-centered design methods (see resources below), to develop ideas to improve health outcomes and reduce inequities among pregnant people.
Developing these ideas is best done with representatives of the population of focus, as they have expertise and experience that may be missing from the practice’s care team. Compensating these patients and community members for time spent on improvement activities is a best practice. During this brainstorm, you are developing ideas without immediate judgment of the ideas in an effort to generate dozens of potentially viable ideas.
9. Determine which strategies to test first.
Suggested team member(s) responsible: Care team and people with lived experience.
Steps seven and eight above help your practice identify existing key activities and generate new ideas.
There are many ways to prioritize ideas. The Institute for Healthcare Improvement (IHI) often recommends a prioritization matrix and/or an impact effort matrix.
If you have organized your key activities and new ideas into themes or categories, you may choose to work on one category or select one to two ideas per category to work on.
The number of key activities and/or new ideas that you prioritize for testing first should be based on the team’s bandwidth to engage in testing. Thus, it is critical to determine the bandwidth for the team(s) who will be doing the testing so thou can determine how many ideas to test first.
10. Use quality improvement (QI) methods to begin testing your prioritized key activities and new ideas.
Suggested team member(s) responsible: Care team and people with lived experience.
Nearly all of the key activities and all of your new ideas will require some degree of adaptation for use within your practice and to be culturally relevant and appropriate to your population(s) of focus.
Whenever testing a key activity or new idea, we recommend that the practice:
- Use plan, do, study, act (PDSA) cycles to test your ideas and bring them to scale. See more information on PDSAs below in the tips and resources section.
- Generally, start with small-scale tests (e.g., test with one patient, for one afternoon, in a mailing to 10 patients, etc.). Use Figure 10 below in the tips and resources section to help you decide what size test is most appropriate. Increase the size of the test as your degree of confidence in the intervention grows.
Develop or refine your learning and measurement system for the ideas you are testing. A simple, yet robust learning and measurement system will help you understand areas for improvement, unintended secondary effects, and how implementation is going.
By working out the inevitable challenges in the idea you are testing in a small-scale PDSA cycle, the ultimate improvement activity will work better for patients and be less frustrating to the care team. Testing and refining also can eliminate the inefficient workarounds that occur when a new process is imposed onto an existing system or workflow without sufficient testing.
Select resources for quality improvement (QI):
- Institute for Healthcare Improvement (IHI) QI Essentials Tool Kit.
- Cause and effect diagrams.
- Driver diagrams.
- Failure modes and effects analysis.
- Flowcharts.
- Histograms.
- Pareto charts.
- PDSA worksheets.
- Project planning forms.
- Run charts.
- Scatter diagrams.
- IHI’s Videos on the Model for Improvement (Part one and Part two).
- Rapid Experiments to Improve Healthcare Delivery.
- CCI’s ABC's of QI via CCI Academy.
11. Educate staff and providers on importance of addressing inequities.
Suggested team member(s) responsible: QI team; care team; patients; diversity, equity and inclusion (DEI) workgroup.
In addition to sharing information from research and data on social inequities, educate staff and clinicians on the existence of social inequities within your organization. Highlight activities that specifically focus on these disparities. Incorporate lessons learned from patients and partner organizations.
Prior to full scale implementation, education can help to ensure buy in from staff and clinicians.
12. Implement – bring to full scale and sustain – those practices that have proven effective.
Suggested team member(s) responsible: Care team
Once an idea has been well tested and shown to be effective on a small scale, it is time for your practice to hardwire the idea, approach or practice into your daily work. Consider using the MOCHA Implementation Planning Worksheet to think through:
- Measurement.
- Ownership.
- Communication, including training.
- Hardwiring the practice.
- Assessment of workload.
Sometimes, implementation may require that you update your protocol and/or policies and procedures for the populations of focus.
13. Once you have tested, refined and scaled up the initially prioritized ideas, begin testing other ideas.
Suggested team member(s) responsible: Care team and people with lived experience.
Consider revisiting the ideas that were developed previously but not were not initially prioritized for implementation. You might also move through the testing steps above to develop and prioritize new ideas or adapt ideas to better serve additional subpopulations of focus.
14. Establish formal and informal feedback loops with patients and the care team.
Suggested team member(s) responsible: Care team and people with lived experience.
Establishing formal and informal feedback loops regarding new processes will ensure that your practice’s ideas are meeting the needs of patients and are reducing identified equity gaps. These feedback loops also ensure the changes are feasible and sustainable for your practice.
For patients, feedback loops could be created using many of the human-centered design tools used to design your improvement activity (e.g., surveys, interviews, focus groups).
Consider establishing a standing funded patient advisory board that is available to design, implement and evaluate all of your practice’s improvement activities.
For the care team, feedback loops might include:
- Existing and new staff satisfaction and feedback mechanisms.
- Regularly scheduled meetings and calls to get staff feedback on processes, methods and tools. Leverage existing meetings to mitigate staff burnout.
15. Continually analyze your data to determine if your efforts are closing equity gaps.
Suggested team member(s) responsible: Care team.
This includes regular (at least monthly) review of the stratified measures for all of the following:
- Core measures for the population of focus.
- Supplemental measures for the population of focus.
- Process measures for the population of focus.
- Social needs data.
- Any additional measures collected as part of your testing and refinement effort.
Share the data with patients to both show your work to decrease known equity gaps and to solicit ideas for closing them.
Implementation tips
When testing a change idea (either a key activity or new idea) for your practice to address a known equity gap, the size of your test is critical. We recommend starting with a very small test (e.g., with one patient or with one clinician) or a small test (e.g., with all patients seen during a three-hour period by this clinician) unless you are certain the change idea will lead to improvement. The cost of a failed small test is extremely low and staff will often be excited to test the change idea. As you learn what is or isn’t working from each test, you can conduct larger scale tests and tests under a variety of conditions. While at first glance this would appear to slow down the implementation effort, starting small and working out the challenges as you progressively work to full scale actually saves time and resources and is much less frustrating for your patients and care team. The visualization below provides guidance on how big your test should be.
FIGURE 10: HOW BIG SHOULD MY TEST BE?
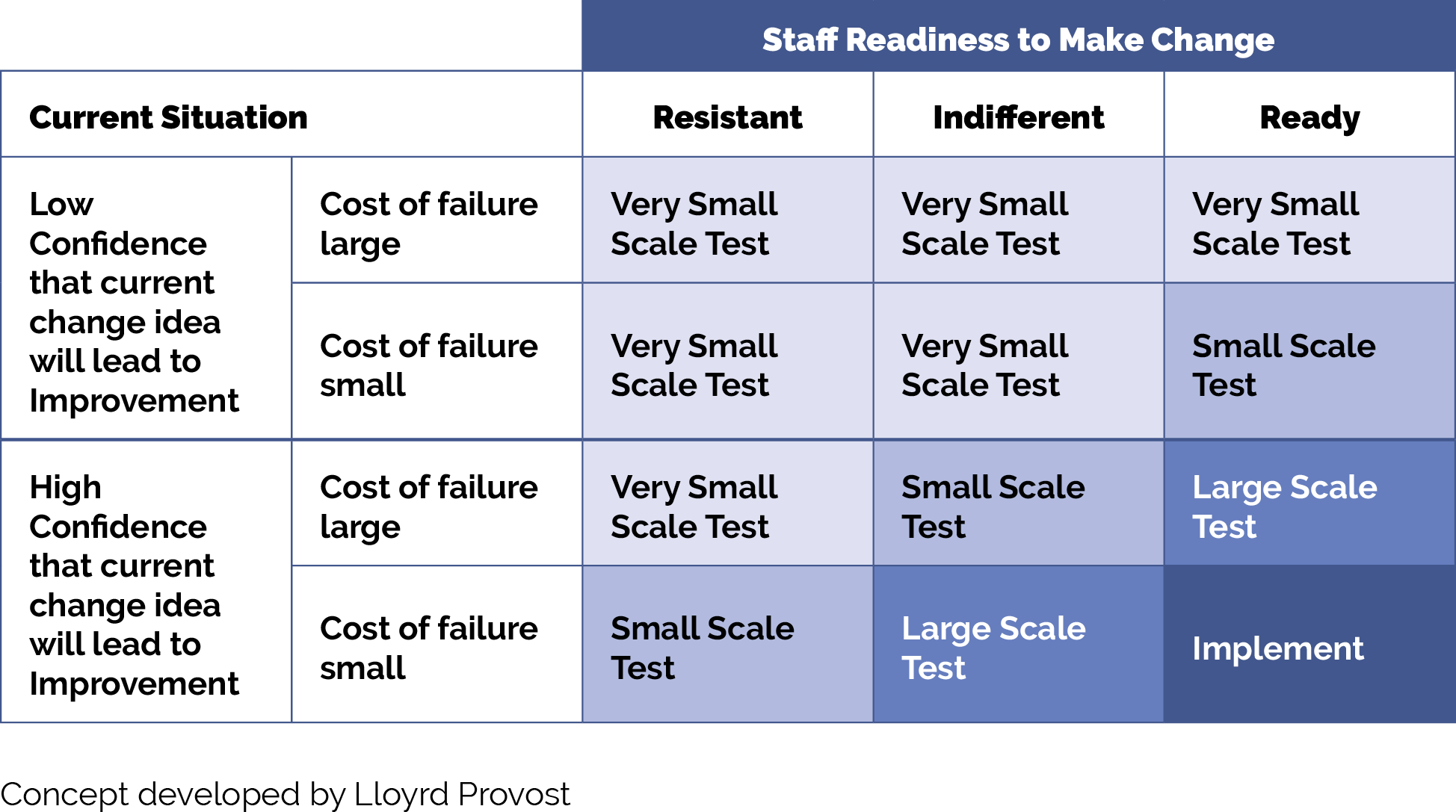
Resources
KEY ACTIVITY #5:
Develop and Implement Standing Orders
This key activity involves the following elements of person-centered population-based care: operationalize clinical guidelines; pre-visit planning and care gap reduction.
Overview
A standing order is a preapproved provider order to perform a specific intervention for any patient who meets the criteria for the order. It is employed by a licensed (LVN, RN) or nonlicensed (MA, health educator) professional when the step in the workflow specifically requires the order of a qualified provider. Standing orders describe the action to be taken and identify who on the care team is authorized to complete the order. Standing orders are designed to enable care team members other than the primary care provider (PCP) to initiate specific clinical actions to provide timely screening and care, provided that specific criteria are met.
An important characteristic of a standing order is that all the patients who meet the criteria for the order receive the same treatment, thereby embedding equality into the clinical approach. Common standing orders include preventive measures, such as immunizations, cancer screenings and other screenings to be conducted ahead of the clinician’s time with the patient. Common standing orders in perinatal include preventive screening guidelines as well as specific testing at certain stages of pregnancy, such as initial pregnancy labs, gestational diabetes screening and group beta strep testing.
To limit the potential for errors and ensure patient safety, standing orders should be carefully designed, regularly reviewed and revised as necessary. They should be based on evidence-based recommendations and best practices, and they should have broad support from the medical director, practice manager, physicians and other staff. In addition, they should outline the criteria for initiating, modifying or discontinuing a particular course of action or treatment for a patient.[13]
Why this matters
Standing orders, in concert with other key activities, allow care team members to work to the full scope of their license and provide scaffolding to support care team members as they work together to support patient care. They promote practice workflow efficiency and effectiveness by standardizing routine care, thus freeing up time for the ordering clinician.
Leveraging this intervention to improve equitable health outcomes
Standing orders help promote equity by ensuring that every patient who meets criteria for an intervention under the standing order is provided with appropriate services, limiting variation that could occur in interpersonal encounters. They follow clinical guidelines to ensure services for pregnant patients are provided at the right frequency based on patient age, gestational duration, pregnancy risk factors and other characteristics. Standing orders empower care team members to initiate these services within their scope and are a best practice tool that enhance the care team’s ability to close gaps in essential services.
Technology Considerations
Most EHRs have the ability to enable the creation of order sets that can be utilized to create standing orders. Order sets are particularly effective for managing a group of standard prenatal orders for a population. (See Appendix D: Guidance on Technological Interventions for more details on implementing order sets in a commercial EHR). Depending upon the health center’s workflows, these order sets can be placed on the chart by providers or can be drawn down by responsible designated staff according to protocols.
For example, a set of obstetric (OB) initial labs can be programmed into the EHR, allowing staff to check a single box to order all the recommended labs at the beginning of a pregnancy.
Relevant HIT capabilities to support this activity include prenatal care guidelines, registries, care gap reports and clinical decision support.
Effectiveness of standing orders can be tracked through registries and care quality reports.
Action steps and roles
The steps below outline the actions required to create standing orders. They are adapted from the University of California, San Francisco (UCSF) Center for Excellence in Primary Care (CEPC).[14]
1. Review and understand the latest clinical guidelines for the required standing order and your practice’s already established protocols.
Suggested team member(s) responsible: Quality improvement lead; panel manager, data analyst, medical director or equivalent.
Interventions specific to the perinatal care population are initiated upon the patient presenting with a positive pregnancy test and indicating they intend to continue the pregnancy. It is recommended that practices ensure access to initial and ongoing perinatal care services through the following best practices:
- As soon as a pregnancy is identified and the patient indicates a plan to continue the pregnancy, practice staff connect the patient with perinatal service staff to initiate prenatal care services.
- Upon notification, perinatal services staff outreach to schedule new prenatal patients for an initial intake visit and a provider visit.
- A workflow is utilized to identify high-risk pregnancies and determine the need for referral to outside specialty obstetrics services.
- If referred, workflow should exist to reengage the patient and new baby after delivery.
- Practice participates in the California Prenatal Screening Program.
- Standing orders are in place for routine prenatal and postpartum testing, including depression screening.
- To maximize completion of postpartum depression screening, the standing order should be executed at the first postpartum visit or integrated within the first well child check with the pediatrician to complete the postpartum depression screen at any visit where the new parent presents. See The Council on Patient Safety in Women’s Health.
2. Translate the appropriate clinical guidelines into a standing order.
Suggested team member(s) responsible: Medical director and panel manager or data analyst.
The standing order will follow the relevant clinical guidelines and be updated whenever clinical guidelines are updated. It will generally allow the following:
- Registered nurses (RNs) and/or medical assistants (MAs) with proper training may initiate the agreed upon standing order process when patients meet the agreed upon criteria for initiating screening, and do not have any clinical history that may require a clinician to address the concern.
- This may include initiating an order, initiating a referral, or notifying the PCP of the need for screening and/or testing.
In addition to the written standing order, the practice should develop a process map or update other documentation outlining how and when the standing order is to be implemented in the practice’s current workflows.
3. Obtain approval for standing orders from clinical leadership.
Suggested team member(s) responsible: Panel manager and/or data analyst and medical director or equivalent.
For the standing order to be valid and in effect, it must be approved by clinical leadership at the practice, signed by a designated valid signatory (e.g., medical director or other physician), and dated, and it must include the effective date for the standing order. Practices should consider including an expiration date and flagging this date in their system to help ensure that the standing order is reviewed and updated regularly. As the clinical guidelines change or other components are updated, the standing order should be signed and dated again by the appropriate party with an effective date for the revision.
4. Train practice staff on how to use standing orders and include this training in clinical onboarding of new staff.
Suggested team member(s) responsible: Medical director or equivalent.
It is critical that practice staff, both those directly named in the standing order and other members of the care team, receive training on the use of this standing order. Such training should include a thorough review of the written standing order and ensure that practice staff understand all of its aspects, including the associated workflow and any additional materials related to the workflow, such as patient education or instructional materials that include nuances that the care team will need to understand.
Training should be provided on each standing order at least annually, retraining should be provided before the effective date on any revisions, and the training should be part of the orientation for all new members of the practice care team.
Based on feedback from the staff, the standing order can be refined to make the instructions clearer (e.g., during training several staff members were confused by a specific instruction, indicating that the instruction needed to be revised).
5. Institute mechanisms to ensure the proper use of the standing order and its effectiveness.
Suggested team member(s) responsible: Clinical director or equivalent or their designee.
It is likely that one or more aspects of the standing order will not work as planned. For example, the practice’s workflow may not fully support the standing order, the wording may be confusing to one or more staff members, or the standing order’s protocol may not be regularly followed exactly (e.g., staff are using workarounds). The practice should routinely check for these and other common challenges and revise and update the standing order as needed to ensure that it works for the practice and meets all applicable regulations and guidelines.
FIGURE 11: COMMON PREGNANCY-RELATED STANDING ORDERS
Standing Order |
Notes |
|---|---|
Initial OB labs |
Typically includes complete blood count (CBC), blood type, Rh factor, rubella immunity, rubeola and varicella immunity, hepatitis B, hepatitis C, sexually transmitted infection (STI) testing (HIV, syphilis, gonorrhea and chlamydia), tuberculosis (if high-risk population), early glucose screening (if high-risk population), and urine culture. |
Depression and anxiety screening |
For prenatal care, patient health questionnaire (PHQ)-2/PHQ-9 is frequently utilized. Screening is often completed at the initial prenatal visit. Edinburgh Postnatal Depression Scale (EPDS) is frequently used for postpartum patients. |
Genetic testing and nuchal translucency |
For more information on the California Prenatal Screening Program: Prenatal Care Providers. Available from: https://www.cdph.ca.gov/Programs/CFH/DGDS/Pages/pns/healthcareprovider.aspx. |
Gestational diabetes screening |
Typically completed between 24 to 28 weeks of gestation. |
Vaccinations |
Tetanus, diphtheria, acellular pertussis vaccine (Tdap): Offered after 28 weeks of gestation with each pregnancy. Influenza: Offered throughout flu season. Respiratory syncytial virus (RSV) vaccination (Abrysvo): Offered at 32 to 36 (or 37) weeks. |
Group B streptococcus (GBS) screening |
If not previously identified in urine culture, rectovaginal swab collected between 36 and 37 weeks of gestation. |
Implementation tips
- The same basic workflow for other standing orders that your practice already has in place can be used as a jumping-off point when developing a new standing order. Before beginning work on a new standing order, determine whether your practice has existing standing orders that you can draw from as you develop this one.
- Verify if carrying out standing orders falls within the legal scope of practice for the supportive clinical staff intended to carry them out. California has very specific guidelines for standing orders for different healthcare professionals, including medical assistants, registered nurses (RNs) and advanced practice clinicians (APCs).
- The first two to four weeks of implementing a specific standing order should be used to test and refine it. We recommend that the practice start with small-scale tests (e.g., test for one day), study the successes and challenges (including errors) of the test, refine the standing order and/or training on it as needed, and then test again, increasing the scale of the test as it results in fewer challenges or errors.
- Common pitfalls of standing orders:
- Standing orders are not updated when screening guidelines are revised and reflect an outdated practice. The remedy is to assign the task of updating the protocols to a member of the team who is responsible for at least annual review and modification.
- New staff are not instructed on the clinical protocols. The remedy is to include review of standing orders as a core element of orientation for all roles named in the standing order.
- Standing orders include the signature of a clinician who is no longer with the practice. Review standing orders at least annually and any time a clinician responsible for setting the order has changed roles.
Resources
KEY ACTIVITY #6:
Develop or Refine and Implement a Pre-Visit Planning Process
This key activity involves the following elements of person-centered population-based care: operationalize clinical guidelines; pre-visit planning and care gap reduction; care coordination; address social needs.
Overview
This activity provides guidance for how the care team can effectively and efficiently implement a pre-visit planning process (PVP).
Pre-visit planning is typically driven by the medical assistant with help from other care team members and includes steps taken:
- At the end of the current visit to ensure the patient understands any actions they need to take and to schedule for any follow-up.
- Prior to a scheduled appointment, to “scrub” the chart and identify any pre-visit tasks per the pre-visit checklist.
- The day of an appointment, during the daily huddle and before the patient sees the obstetric provider.
Why this matters
The average prenatal care visit at California practices lasts just 10 to 15 minutes, and many patients come to these visits with multiple needs. Pre-visit planning works towards optimizing a team-based approach so patients receive comprehensive care in alignment with the latest clinical guidelines and their own needs and preferences.
Leveraging this intervention to improve equitable health outcomes
Pre-visit planning allows for better coordination of care. This can be particularly beneficial for patients with complex, higher risk pregnancies, ensuring they receive comprehensive and equitable care. As your practice works to reduce any identified equity gaps, pre-visit planning is often a powerful activity for ensuring relevant care as the care team partners with the patient to discuss important screening or testing due at the time of the visit.
Leveraging this intervention to help address patients’ social needs
The PVP should incorporate your practice’s process for screening and responding to social needs, including checking whether social needs screening is due. When social needs are identified the team should be clear on the pathways, both during and after visits, to address and follow up on those needs.
Technology Considerations
Pre-visit planning draws upon similar technical enablers as care gap reporting, and likewise can be facilitated at the individual patient level and at the level of groups of patients coming for care by a specific team in an appointment schedule block. The format in which planning is done needs to consider the workflow and staffing model.
Individual patient level pre-visit planning would optimally be enabled within the EHR, provided the EHR is able to store relevant information such as assessments, plans, orders and notes outside of a visit note. Pre-visit planning might also include use of patient-facing applications such as portal reminders, questionnaires and self-completed screenings and assessments, which ideally would be available to the provider and care team in the EHR.
Engagement of the expanded care team in pre-visit planning requires access by all relevant members of the care team to contribute to and view relevant information. This may require coordination with technology additional to the EHR, such as care coordination and population management applications where relevant information might be stored.
Huddle reports, in which individual patient information can be visualized in summary views across all patients within a session, can require use of technology outside the EHR, but might also be supported by developing reports populated by data from the EHR. Ideally, internal practice and EHR data should be supplemented with external data where such information completes the patient’s current status. Establish access to local hospital systems to obtain prior pregnancy and delivery records. Standardize where these records are inputted into the EHR. If such electronic access is not possible, workflow should include manual reconciliation by history from the patient. Relevant HIT capabilities to support this activity include prenatal care guidelines, registries, clinical decision support, care dashboards and reports, outreach and engagement, and care management and care coordination.
See Appendix D: Guidance on Technological Interventions.
FIGURE 12: AN EXAMPLE OF HOW TECHNOLOGY CAN HELP WITH PRE-VISIT PLANNING
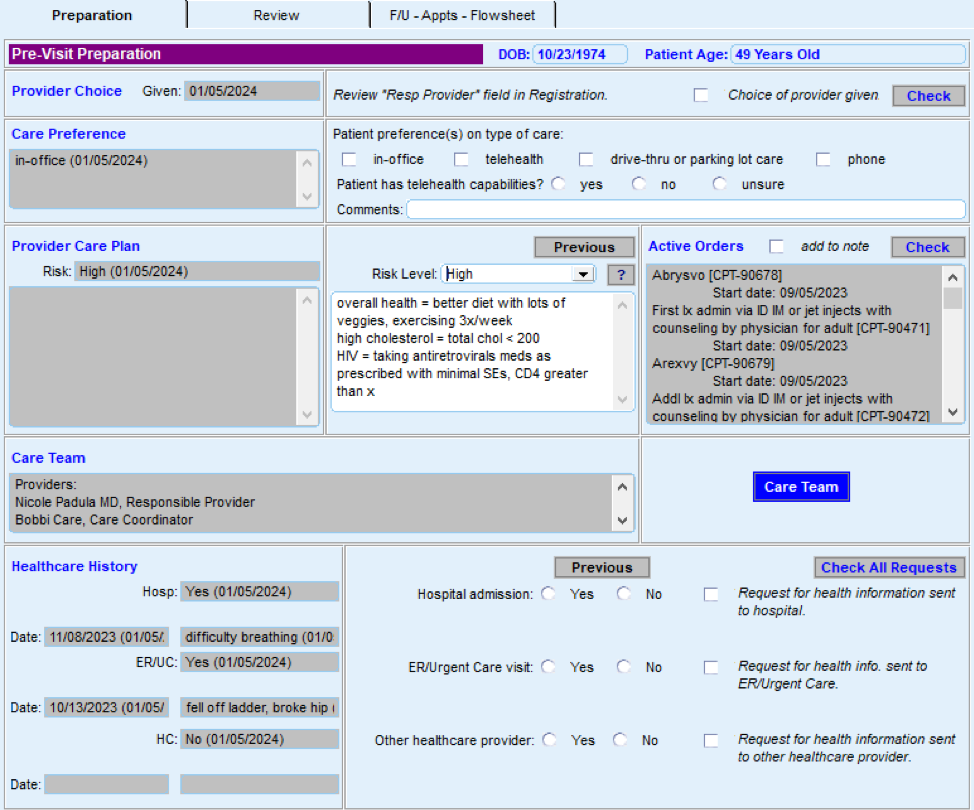
Action steps and roles
1. Assess the current state of the pre-visit planning (PVP) process across your practice.
Suggested team member(s) responsible: Implementation team or QI team.
Understand how the process currently works for prenatal and postpartum care in light of your practice’s performance on core and supplemental measures. Compile existing paperwork and process documentation into one place and talk to medical assistants and other members of the care team to understand their questions and challenges around the pre-visit planning process.
Consider making current-state process maps that communicate the major steps in the PVP process and acknowledge pain points or challenges in the process. Pain points are places where the process isn’t working well for patients, staff or specific subpopulations or demographic groups for which your data analysis has revealed equity gaps. In addition, pay attention to places where staff are creating workarounds to the process. The presence of workarounds indicate that the process might need further clarification or refinement to support the care team to reliably implement it.
Your team may find it helpful to compile process maps for both the high-level pre-visit planning as detailed in Figure 13 in addition to more detailed documentation for specific clinical workflows.
FIGURE 13: PRE--VISIT PLANNING (PVP) WORKFLOW EXAMPLE
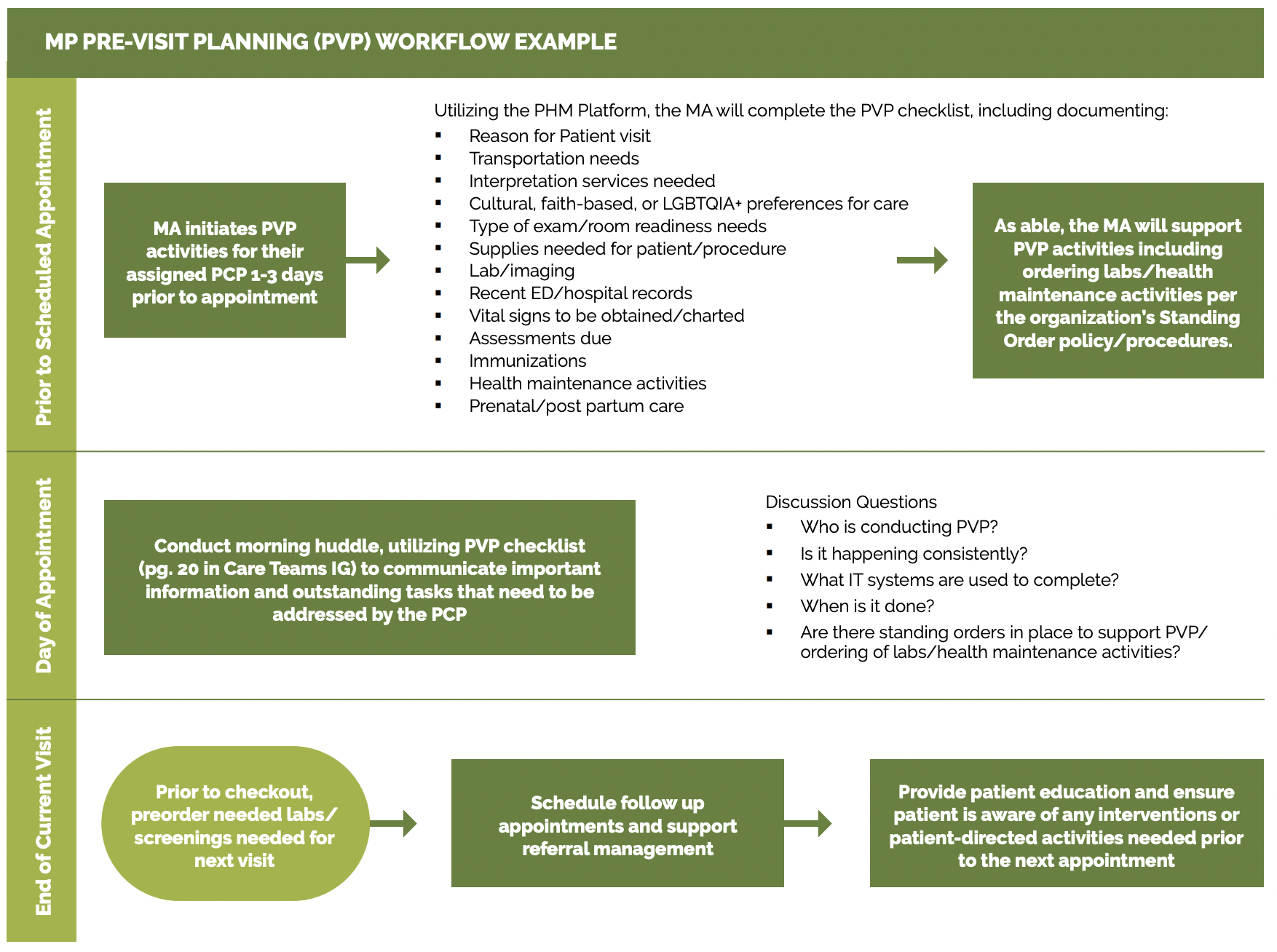
2. Identify where to update the PVP process to more consistently and reliably address care gaps.
Suggested team member(s) responsible: Implementation team or QI team. May include the data manager to assist with identifying patients through EHRs.
Examine where you can further incorporate or streamline your practice’s clinical protocols and standing orders into PVP, including via the PVP checklist, daily huddles and other key clinical workflows. Examples and considerations for updating the PVP process are included below.
Patient provider continuity is associated with better patient and provider satisfaction. Determine if the PVP process can be leveraged to improve provider continuity for perinatal patients.
Clinical guidelines and care gaps: Consider which preventive and maintenance services could be addressed more reliably using PVP, including those in your EHR’s care gap module. The Pre-Visit Planning: Leveraging the Team to Identify and Address Gaps in Care resource provides a more complete list of preventive services for adults and children.
PVP checklist: A generic PVP checklist to be completed by the MA or licensed vocational nurse (LVN) at least one to three days before the appointment is provided in Figure 14. Most EHRs will have a health maintenance module that identifies what preventive care is due, but a printed or digital checklist provides a starting point for ensuring key steps aren’t missed. For prenatal or postpartum care, the PVP checklist should include checklist items directly relevant to obstetric services. One approach is to create trimester-specific checklists to guide the MA or LVN in identifying key information.
FIGURE 14: PRENATAL AND POSTPARTUM PVP PLANNING CHECKLIST
Checklist Domain |
Checklist Item |
|---|---|
General |
|
Room readiness |
|
Pregnancy history and current problem list |
|
Medical record review |
|
Assessments needed |
|
Care gaps |
|
For postpartum visits |
|
Daily huddles: Design or redesign the team’s daily huddle so the care team can review prioritized action items for the list of patients scheduled to come and any further follow-up for patients seen in the previous days. For more information, see the Care Team and Workforce Guide Resource 4: Daily Huddles Overview and Process.
The Center for Excellence in Primary Care resource on healthy huddles includes tools, a video and examples around how pre-visit planning flows into the daily huddle process, including a healthy huddle warm-up, which can help MAs prepare for huddles.
Patients requiring special considerations: Ensure that the PVP includes a process to flag for the care team:
- Patients requiring special attention, such as those with:
- Chronic conditions impacting their pregnancy.
- Conditions that require increased coordination with specialty care or other services (e.g., patients with gestational diabetes).
- Complex psychosocial needs.
- Recent hospitalizations.
- Patients who need extended time or additional services during their visit (e.g., translation services, mobility assistance, screenings).
Detailed clinical workflows: Clinical workflows should be updated to describe at which step in PVP or the patient visit a care team member will address a specific gap in care with the patient. This may include the following details:
- Who will initiate the discussion with the patient based on the needs (e.g. preferred language) and preferences of the patient.
- How and when the care team member will plan to have the discussion before, during or after the visit.
- How they will be prepared to address common barriers or concerns the patient may have.
- Educational materials available for use that are relevant to the patient.
Planning for care after the visit: Effective PVP includes scheduling pre-visit labs and other diagnostics at the end of the current visit and coordinating care and referrals for services not available at the practice. See Key Activity 13: Coordinate Care for more information. Confirm the patient understands the purpose of any follow-up care.
The American Medical Association (AMA) has an online guide for implementing pre-visit planning, which includes forms, templates and other resources.
3. Test planned changes to the PVP workflows and support care teams in implementing the workflow.
Suggested team member(s) responsible: Implementation team or QI team.
Test and refine important changes to the PVP process with one or two care teams before considering rolling out the change more broadly at the practice.
Implementing the change includes updating documentation and creating a staff training schedule or training refresher for staff to sustain workflow changes. For example, train MAs every six months on the PVP. If they have difficulty, have them retake training with a different highly effective MA and monitor closely until competency in the task is reached.
For further streamlining of the process, practices can customize EHR templates to align with PVP workflows. Be sure to account for potential costs associated with creating new templates, staff training and IT.
4. Establish a process to review and update PVP workflow.
Suggested team member(s) responsible: Care team with quality improvement manager.
Identify staff responsible for reviewing and updating the PVP process at least annually to incorporate the latest clinical guidelines and check for any workarounds that have developed.
Resources
KEY ACTIVITY #7:
Use Social Needs Screening to Inform Patient Treatment Plans
This key activity involves the following elements of person-centered population-based care: behavioral health integration; address social needs.
Overview
This activity provides guidance on screening patients for health-related social needs and how the information can begin to be used to inform patient treatment plans, including referral to community-based services. Social needs are defined as individual material resources and psychosocial circumstances required for long-term physical and mental health and well-being, such as housing, food, water, clean air, sanitation and social support.
Why this matters
Evidence continues to accumulate that demonstrates the ways in which social needs impact physical and mental health outcomes. This is particularly true for pregnant and postpartum individuals and their families. The relationship is not unidirectional. Worsening physical and mental health conditions have also been shown to impact social stability.[15]
Health-related social needs and unmet social needs are known to be related to a variety of perinatal outcomes: unintended pregnancy, preterm birth and maternal mortality. Your practice must recognize that a patient’s pregnancy and postpartum care decision-making is shaped by larger systems and life circumstances. Screening for and addressing social needs will help your practice better understand the populations you serve and improve their birth outcomes.[16]
Leveraging this intervention to improve equitable health outcomes
Discrimination related to race and ethnicity, immigrant status, sexual orientation and/or occupational status has repeatedly been associated with negative mental and physical health outcomes.[17] Providing healthcare in the absence of attending to the life circumstances in which patients and their families are living risks doing harm rather than providing assistance or support.
Here are some places to start to integrate equity and social needs work:
- Identify and agree to use a specific social needs screening tool. Test this tool and develop processes to use it consistently.
- Hire and train behavioral health staff who are skilled at discussing and incorporating the impacts of racism on individual mental and physical health.
- Social needs screening often asks questions about private and potentially stigmatized aspects of a patient’s life (e.g., poverty and inter-partner violence).[18] Ensure staff are trained to screen for and respond to social needs in a trauma-informed way (See the Resource: Trauma-Informed Population Health Management)
- Integrate demographic data with chronic disease and social needs data. Too often such data is siloed in the EHR and requires staff and organizations to intentionally consider opportunities to integrate and report out such data.
Leveraging this intervention to help address patients’ social needs
Social needs screening is an opportunity to both make visible the factors outside of the clinic that greatly impact patients’ health and to connect and link patients and their families with appropriate resources to meet those needs. Care teams reflect on screening results to tailor adjustments, such as prescribing or location/timing of visits, to individual care plans. Considering the intertwining of social needs with physical and behavioral health allows care teams to reflect on root causes and can lead to improved individual and collective health outcomes.
Note: There is not yet consensus or uniform endorsement regarding screening for social needs, due at least in part to a lack of high-quality evidence on the risks, benefits and best practices of screening and response.[19] For example, findings from the recent Centers for Medicare and Medicaid Services (CMS) Accountable Health Communities Model indicate that the social needs screening and navigation services reduced ED utilization and may have reduced expenditures but did not appear to increase patient’s connection to community services or resolve the patient’s social needs.[20] Other possible ways social needs screening can support attending to social needs include by strengthening the patient/provider relationship,[21] destigmatizing social services, tailoring care and, at a population level, increasing social investment.[22]
Technology Considerations
Technology-enabled screening referenced in the technology section can be utilized to screen patients for social needs through the channels described: directly in the EHR, in applications used by care coordinators, and directly to patients via patient-facing outreach and engagement technologies. Examples of screenings include depression/anxiety, substance use disorder, health related social needs and domestic violence, to name a few.
Health centers will need to determine a strategy to ensure that externally generated screening information be incorporated into the patient record, recognizing its impact on care delivery for pregnant people, risk assessment and management, and for managing relevant referrals. Social health information exchanges exist in some communities to identify where patients are getting social services and help identify higher risk patients. These will develop over time.
Action steps and roles
1. Pick a validated standardized screening instrument and establish how to document results.
Suggested team member(s) responsible: Clinical leadership.
Pick a standardized screening tool that fits your organizational environment and the context of your patient population. Kaiser Permanente, in partnership with the Social Interventions Research and Evaluation Network (SIREN), conducted a systematic review of social needs screening tools and provides a comparison and search tool for different tools for adults and children. Currently available standardized tools you might consider include:
- Protocol for Responding to and Assessing Patients’ Assets, Risks and Experiences (PRAPARE) developed by the National Association of Community Health Centers (NACHC).
- The Centers for Medicare and Medicaid Services (CMS) Accountable Health Communities (ACH) screening tool.
- REACH by Health Leads.
- The Academy of Family Practice (AFP) tool.
For the perinatal population, it is especially important to assess the safety of the pregnant person from intimate partner violence and determine if any intervention or support is needed. Consider a validated tool that has comparable questions found in the California Comprehensive Perinatal Services Program (CPSP) intake assessment.
Work with your clinical informatics team to determine how staff will document screening results in your EHR. Some EHR systems have screening tools already embedded and many are moving quickly to incorporate screening; some EHRs may be able to auto-populate Z-codes based on screening results. Your managed care plans may offer additional guidance or support and can be a resource to connect your practice to other organizations who have experience with screening instruments and technology tools. By using the same screening tools and/or information technology platforms, the consistency and quality of care delivery can be enhanced.
For the patient’s problem list, Department of Health Care Services (DHCS) provides a list of 25 Priority Social Determinants of Health (SDOH) Codes to focus on. This shorter list of codes is intended to capture areas where the health system may have the greatest impact on identifying and addressing social needs. Train providers to add these codes to the pregnant patient’s problem list as appropriate.
2. Understand resources and community referrals for positive screens.
Suggested team member(s) responsible: Referral manager, community health workers.
Through CalAIM, the California Department of Healthcare Services (DHCS) has taken steps to ensure that Medi-Cal members have access to social support that can impact health outcomes. Connect with your managed care plan (s) (MCPs) and regional area consortia (RAC) to understand what services and resources they have in place to support patient access to community-based social services. Many MCPs are developing relationships with social services agencies to meet the needs of their members. For Medi-Cal members with the highest level of social needs, MCPs offer Enhanced Care Management (see section on care management) and some or all of 14 Community Supports: these Community Supports provide resources to address social needs such as housing navigation, post-hospitalization recuperative care, and medically tailored meals. Some MCPs use the new CalAssist tool for Medi-Cal members to self-identify whether they are eligible for any of the 14 CalAIM Community Supports and generate a referral to the applicable community support provider.
Beyond these relatively new benefits that may meet the social needs of your pregnant and postpartum patients, your practice may also refer to existing community-based organizations and public agencies to support patient needs like nutrition assistance, employment readiness, childcare support, postpartum paid family leave, rent and utility assistance, and resources for transportation. Existing free social support programs for your pregnant and postpartum patients include California Home Visiting Programs and home visitors (public health nurses or peers) who are well-versed in meeting patient social needs. Such existing programs, often administered by your local public health department in partnership with community-based organizations, should be leveraged where possible to support new social needs screening and response processes in your practice.
Many patients will screen positive for social needs and will benefit from connection to alternative resources that are not part of Community Supports. Contact your MCP to see if they have established relationships with providers who connect individuals to social services. Health plans may contract with an online provider or with a social services network lead entity that can connect you with existing community-based organizations and public agencies in the area. These contracted services will often include a process for making closed loop referrals, where the referring provider is notified if the patient has successfully accessed the referral. Closed loop referrals are a best practice in care coordination that lead to higher levels of patient and provider satisfaction.[23]
Key services to catalog include nutrition assistance, employment readiness, childcare support, postpartum paid family leave, rent and utility assistance, and resources for transportation. Other places to look to build sources for local community referrals include:
- Your current social work staff and/or community health workers, who may have many go-to resources already identified.
- Free online aggregators for local community services in California, such as findhelp.org.
- 2-1-1 a free telephone number providing access to local community services for housing, utility, food and employment assistance.
- Resource networks maintained by a local hospital or larger health system in your area.
For going deeper in this area, practices can consider prioritizing quality improvement activities that establish new or previously underutilized community resources to address specific social needs as part of Key Activity 4: Use a Systematic Approach to Decrease Inequities within the Population of Focus. Case studies provided in the resources linked below provide examples of these improvement initiatives.
3. Establish a workflow for screening and referrals.
Consider screening before the patient meets with the PCP and have a workflow in place for follow-up of positive screen (e.g. meet with care coordinator or care management staff who will facilitate referral). Take steps to flag the positive screen so the PCP is aware and can address any positive screen during the visits.
Train staff in the new workflows and Implementing Population Health Management in Trauma-Informed Ways. Staff often initially resist screening if there is a sense they feel they don’t have the tools to help address positive screens.
- Following screening, ask patients for their prioritized need and whether they would like assistance before making a referral.
- Providing a written script for staff and accompanying signage can build confidence in dealing with the challenging circumstances many patients experience.
4. Provide person-centered care that acknowledges social needs.
Suggested team members responsible: PCPs and the expanded care team.
Information about a patient’s social needs can be used to provide tailored person-centered care and treatment plans that patients are more likely to follow. For example, if a patient screens positive for food insecurity, that could influence details around dietary advice given for pregnancy. If a patient screens positive for transportation insecurity, discuss what options might be available to ensure proper access to appointments. Use trauma-informed ways of engaging patients in their own care, including developing shared goals, providing self-management support, and using communication techniques such as motivational interviewing. See more here: Implementing Population Health Management in Trauma-Informed Ways
The desires and goals of the patient will inform how and when to move ahead in addressing social needs. It is important to support patients through motivational interviewing and trauma-informed practices to create a person-centered care plan. By having processes in place to support ongoing person-centered care planning, such as a warm handoff to a care coordinator or a documented plan to follow up on issues discussed at the next visit, will help to build trust and support connection to community referrals when the patient is ready.
Example of how this activity has been implemented
Rogue Community Health Center in Medford, Oregon, recognized the need to implement screening for health-related social needs. They also recognized that the lack of interoperability of health information flow was a barrier to collaboration in their community. As a result, they served as a convener and backbone partner, pulling together a group of community-based organizations and public health entities into a “no wrong door” model for screening of social needs. The partnership was called the Rogue Challenge and resulted in a shared community database where patients could be screened at multiple data entry points and the life cycle of a positive screen and referral could be tracked to ensure that people with positive screens were connected to community resources and completed their referrals. Together, the collaborating partners selected an appropriate validated social needs screening tool and adapted it to their context. Next, the team tested screening workflows, including the ability to access information and provide additional screens. This approach expanded the capacity of community-based organizations to administer social health screening, which provided the health center with information in advance of a clinic visit. In their value-based care environment, it had the added benefit of identifying new patients not connected to primary care and connecting them to the health center, thus growing their population of capitation patients.
Implementation tips
- Following screening, ask patients for their prioritized need and whether they would like assistance before making a referral.
- Health-related social needs such as food, housing, and income insecurity can contribute to unhealthy behaviors and lifestyles that contribute to the development or worsening of disease processes during pregnancy. For example, lack of access to nutritious foods may impact a pregnant patient’s ability to manage their gestational diabetes. It is important to screen pregnant people for those social needs, as it may be challenging to deal with their conditions until their social needs are resolved.
- Food and income insecurities are contributing factors to many chronic conditions. Assisting patients with good food choices and sources can contribute to their well-being. The stigma of using community resources for food insecurity can be a barrier to some. Providing a goodie bag of food and connecting the patient to the local food support (see Medi-Cal program supports) can help overcome the stigma while empowering staff.
Resources
Examples from the Center for Care Innovation (CCI)
Case studies of how practices implemented screening tools and undertook innovative quality improvement activities to address food insecurity and transportation insecurity.
Addressing Food Insecurity: Concrete Advice From Clinic Leaders
Food Insecurity: Hidden Hunger in Los Angeles
Addressing Transportation Insecurity: Concrete Advice From Clinic Leaders
Recommended additional social health assessment tools for the prenatal care population.
KEY ACTIVITY #8:
Provide Prepregnancy Healthcare
This key activity involves the following elements of person-centered population-based care: proactive patient outreach and engagement; pre-visit planning and care gap reduction.
Overview
This activity provides guidance on delivering effective prepregnancy healthcare. The CDC and U.S. Office of Population Affairs describe preconception as any time that a person of reproductive potential is not pregnant but at risk of becoming pregnant, or when a man is at risk for impregnating his female partner.[24] While many organizations and agencies still utilize the term “preconception,” there is increasing adoption of “prepregnancy care” as alternative language.[25] Prepregnancy health services aim to identify and modify biomedical, behavioral and social risks to an individual’s health or future pregnancy outcomes through prevention and management. Individuals of reproductive age should receive services tailored to their unique needs before getting pregnant (prepregnancy health services) or between births (interconception health services).[26] Based on the unique needs identified, healthcare providers should suggest a treatment plan or follow-up care as needed.[27]
Why this matters
Prepregnancy health services are beneficial because of their role in improving the health of individuals of reproductive age across their lifespan, regardless of whether they are planning a pregnancy and because of their effect on pregnancy and birth outcomes, especially for people with preexisting health conditions. These services help to reduce pregnancy-related adverse outcomes, such as maternal morbidity and mortality, low birth weight, preterm birth, and infant mortality. Prepregnancy health services are particularly important given that, according to the Centers for Disease Control and Prevention (CDC), almost half of all pregnancies in the United States are unintended.[28] Since many people do not actively plan a pregnancy, focusing on overall prepregnancy health and well-being allows individuals to be prepared for a healthy pregnancy if it does happen. CDC recommends that prepregnancy health services be integrated into primary care visits for all individuals of reproductive age.
Leveraging this intervention to improve equitable health outcomes
In 2021, the maternal mortality rate for non-Hispanic Black women was 69.9 deaths per 100,000 live births, 2.6 times the rate for non-Hispanic white women (26.6). Rates for Black women were significantly higher than rates for white and Hispanic women. These disparities identify an opportunity for significant improvement, as per the CDC. Research indicates that contraceptive services in the year before conception and routine exams for women with chronic disease are associated with decreased odds of severe maternal morbidity or death for Medicaid enrollees.[29] Prepregnancy care, in addition to quality prenatal and postpartum care, helps to ensure good health outcomes for birthing people and infants. Prepregnancy services present a critical opportunity to address modifiable risk factors that contribute to poor birth outcomes for birthing people and infants, both before pregnancy as well as between pregnancies.[30]
Leveraging this intervention to help address patients’ social needs
The American Academy of Pediatrics (AAP) and the American College of Obstetricians and Gynecologists (ACOG) identified four categories of interventions and eight areas of screening for preconception health services. Two of these areas present opportunities to attend to the social needs of patients, including psychosocial concerns such as depression or violence.[31] The four categories of interventions are physical assessment, risk screening, vaccinations and counseling. Eight areas of risk screening are 1) reproductive awareness; 2) environmental toxins and teratogens; 3) nutrition and folic acid; 4) genetics; 5) substance use, including tobacco and alcohol; 6) medical conditions and medications; 7) infectious diseases and vaccination; and 8) psychosocial concerns (e.g., depression or violence).
Technology Considerations
This activity entails the promotion of education, screening and appropriate care to people of childbearing age, and therefore should entail support through all relevant care activities.
Relevant health information technology (HIT) capabilities to support this activity include documentation of medical and surgical histories; routine women’s health, prepregnancy and prenatal care guidelines; care gap reports; SOGI; social needs and SDOH assessments provide information necessary to support comprehensive preconceptual healthcare for individual patients. Data can be available in the EHR or can be collected and integrated into the patient record. Ideally, clinical decision support can inform many care and screening needs, when available (EHR capture is il). Standing orders can be created to support pregnancy care requirements.
Action steps and roles
1. Assess current preconception health services to identify gaps between current and recommended practices.
Suggested team member(s) responsible: Population health staff, care managers, data analysts, all care team members.
Review current preconception health evidence-based guidelines and recommendations. Determine if the recommended eight areas of risk screening for preconception health services are in place. Based on assessment findings, develop and implement a quality improvement plan over time. Your practice might want to start with a focus on one specific process change to support prepregnancy health that might be most impactful in your patient population.
2. Ensure prepregnancy health assessments incorporate social health.
Suggested team member(s) responsible: All care team members.
Incorporate life course theory into preconception health assessments. Life course theory describes how contextual and environmental factors inform individuals’ health across their lifetimes and shape health and disease patterns across populations and communities. Before counseling a client about healthy behaviors, providers should routinely assess the client’s context and environment.
Balanced information on risks and benefits should be presented:
- Preconception Health Toolkit.
- National Preconception Health and Healthcare Initiative: Women’s Health Practice Bulletin 2020
- Providing Quality Family Planning Services: Recommendations of CDC and the U.S. Office of Population Affairs
- Client-Centered Reproductive Goals and Counseling Flow Chart (parenthood and pregnancy attitude, timing, and how).
See Key Activity 7: Use Social Needs Screening to Inform Patient Treatment Plans.
3. Routinely assess all patients’ reproductive goals.
Suggested team member(s) responsible: All care team members and patients.
A standardized and systematic approach is recommended to assess patients’ reproductive goals.5 A standardized approach can decrease bias and inequity in screening and service provision.
PATH (Parenting/Pregnancy Attitudes, Timing, How Important) questions are one client-centered approach to assess parenthood and pregnancy attitude, timing, and pregnancy prevention.
PA: Do you think you might like to have (more) children at some point?
T: When do you think that might be?
H: How important is it to you to prevent pregnancy (until then)?
PATH can be used with clients of any gender, sexual orientation or age. PATH is designed to facilitate listening and efficient client-centered conversations about preconception care, contraception and fertility, as appropriate.
To adapt for EHR, a screening question can be, “Do you think you might like to have (more) children any time soon?”
Another option is One Key Question®. One Key Question® (“Would you like to become pregnant in the next year?”) can be used by healthcare providers, community health workers and home visiting nurses to guide a conversation with patients on a routine basis about pregnancy desires and goals and offer personalized counseling and care based on their response.[32] The One Key Question® is person-centered as it guides a conversation, supporting those who want to get pregnant, those who do not and those who are uncertain.7 One Key Question® (“Would you like to become pregnant in the next year?”) has four possible answers (there is no right or wrong answer): “Yes,” “no,” “unsure,” or “OK either way.”5 The benefits are its simplicity and ability to easily incorporate into routine intake questions and EHR workflows. The question of, “How important is preventing a pregnancy to you?” should also be explored.5
The importance of standardizing: All patients benefit from prepregnancy health services. Following a standardized and systematic approach to assessing patients’ reproductive goals can decrease bias and inequity in screening and service provision.5 Establishing effective referrals systems and making referrals based on identified needs ensures promotion of whole-person care.
4. Assess risk factors for adverse health and adverse pregnancy outcomes before conception.
Suggested team member(s) responsible: All care team members.
The goal of preconception (or prepregnancy) care is to optimize health outcomes by providing education and addressing modifiable risk factors.2 Any visit with a client who has reproductive potential is an opportunity for prepregnancy counseling. After a discussion of the client’s reproductive desires, a prepregnancy counseling conversation can be introduced, if relevant, with: “Since you said ______, would you like to talk about ways to be prepared
for a healthy pregnancy?” For example, the Preconception Counseling Checklist.
5. Make appropriate referrals based on the prepregnancy counseling conversation and assessment.[33]
Suggested team member(s) responsible: All care team members.
Referral and communication pathways between healthcare providers, community-based organizations, and state and public health agencies can enhance access to, and utilization of, services and supports for patients.
Making referrals encompasses a spectrum of potential information-giving and supportive behaviors ranging from providing information on specific services to follow-up on service utilization and outcomes and assessment of the quality of referrals. “Cold” and “warm” are often used to describe referral behaviors at two points along this spectrum. A cold referral means providing information to the client about another agency or service, and it is then the client’s responsibility to contact the agency or service. A warm referral involves contacting another agency or service provider on the client’s behalf. This entails calling and making an appointment for the client, viding support to overcome barriers to care, and following up to determine if the appointment has been kept.
6. Strengthen the quality and responsiveness of prepregnancy health services.
Suggested team member(s) responsible: All care team members.
Unique factors affect each client’s health. Health centers should provide prepregnancy health education, counseling, care and referrals that align with evidence-based guidelines and take into account the goals, risks, social needs, and contextual and environmental factors gathered during a client’s prepregnancy health assessment.
7. Collaborate with community partners to improve preconception health.
Suggested team member(s) responsible: All care team members, community health workers, outreach workers and navigators, community partners, and patients.
Although improving the quality of prepregnancy health services in the clinical setting is important, it is insufficient for reducing maternal morbidity and mortality at scale. Local and national agencies and local birth-centering programs must work together to address social needs, which drive health inequities within communities of color and increase their burden of poor health outcomes. Engaging in diverse collaborative community partnerships can help family planning agencies identify additional opportunities for improving maternal health outcomes.
For going deeper in this area, please see Key Activity 18: Strengthen Community Partnerships.
KEY ACTIVITY #9:
Conduct Postpartum Planning and Care
This key activity involves the following elements of person-centered population-based care: operationalize clinical guidelines; implement condition-specific registries; proactive patient outreach and engagement; pre-visit planning and care gap reduction; care coordination; behavioral health integration; address social needs.
Overview
This activity provides guidance on conducting effective postpartum planning and care. Postpartum care is a critical part of the reproductive healthcare continuum.[34] The postpartum period is a vulnerable time for patients from both physical and mental health perspectives: most pregnancy-related deaths in California occur during the postpartum period[35], and pregnancy-associated mood disorders are the most common comorbid conditions in the perinatal period[36]. Optimal postpartum care should be an ongoing process with, at minimum, two visits completed by three and 12 weeks after birth. The timing and frequency of postpartum visits should be tailored to a patient’s individual health concerns and needs[37] (e.g., adding a visit in the first seven days for a blood pressure check, modifying the schedule to allow for contraception method initiation, or increasing the frequency of follow-up visits for a mood concern).
Care during the postpartum period should include other preventive health screenings and services a patient might be due for, such as depression screening, substance use screenings, cancer screenings and immunizations. Additional elements of optimal postpartum care include screening for social needs and linkage to specialty care and services; certifying paid family leave; management of pregnancy-specific health conditions; anticipatory guidance addressing the transition to parenthood and well-person care; comprehensive contraceptive services; and interconception counseling. Postpartum visits present a good opportunity to discuss interconception care[38]; the provider and patient can reflect on any birth complications and discuss modifiable risk factors that might improve subsequent birth outcomes (e.g., monitoring for recurrence of preterm birth and aspirin to prevent recurrent preeclampsia). Although the postpartum period begins after birth, the postpartum transition may be experienced for six months or more; therefore, planning for this important period, or “fourth trimester,” should begin during pregnancy.[39]
Why this matters
Maternal mortality in the United States is far higher than in other developed nations, and it continues to rise. In California, maternal deaths are disproportionately high in the birthing population insured by Medicaid.[40] In addition, significant racial disparities in health outcomes exist for pregnant and postpartum patients. More than 50% of pregnancy-related deaths occur one week to one year after pregnancy, and more than 80% of pregnancy-related deaths are deemed preventable. Currently, up to 40% of birthing people do not attend a routine postpartum visit, and few receive all recommended elements of postpartum care. The postpartum period provides an important opportunity to support birthing persons and their families, as it is often a time of increased patient motivation, engagement and access to insurance. Intervention in the postpartum period can contribute to long-lasting maternal health and family benefits. It is therefore critical to ensure that birthing persons receive comprehensive care and support during the postpartum period.
Leveraging this intervention to improve equitable health outcomes
These strategies are equity-based interventions.
Developing your postpartum care pathway presents an opportunity to improve equitable health outcomes. For example:
- When you stratify your quality performance data on postpartum visit completion, you might find lower performance in certain subpopulations. Consider focused outreach strategies or creative ways of reaching these patients to schedule and confirm postpartum visits.
- Certain serious pregnancy and postpartum complications disproportionately affect patient subpopulations experiencing marginalization (e.g., hypertensive disorders of pregnancy among individuals who identify as Black or African American). Focusing postpartum process improvements on these conditions and subpopulations may close disparity gaps in process measures while meaningfully supporting safer births (e.g., ensuring all patients with hypertensive disorders in pregnancy have early postpartum visits and medical equipment for close blood pressure monitoring).
- Ensure that your clinic’s postpartum visit scheduling processes do not create unintentional obstacles to accessing contraception (e.g., requiring separate visits for contraceptive placement procedures).
- Breastfeeding has well-established health benefits for postpartum individuals and their infants. Rates of breastfeeding initiation and continuation may be lower in your practice among certain already marginalized groups. Ensure that proactive lactation education and supplies are provided in these groups.
Leveraging this intervention to help address patients’ social needs
Good equity-based interventions attend to patient and family needs and are whole-person centered. The postpartum visit lends itself well to administering a comprehensive social needs screening as discussed earlier in this implementation guide. There are specific focus areas and activities you can consider to attend to some common social needs specific to the postpartum population:
- Postpartum patients and their families may qualify for nutrition support through state and federal programs. Ensure that linkages to these programs are automatically provided for eligible patients.
- Job protections and income support are key during the postpartum period. Ensure that your patient, if eligible, applies for paid family leave. Train staff on this benefit and ensure they are ready to provide certification.
- Refer interested and eligible clients to programs that provide holistic postpartum support: home visiting, doula services, and community health worker services.
- Link to ongoing social needs, including access to transportation, childcare and dyadic services.
Technology Considerations
This activity relies on similar capabilities as care gap management, utilizing population views and registries to track patients who have delivered and should be scheduled for a postpartum visit. These registries can be utilized to generate outreach lists for appointment schedulers and/or care managers and other care team members who might be tasked with contacting patients. Many EHRs are capable of storing next appointment data that can also be used to generate lists and may link to automated appointment outreach workflows. Patient-facing outreach and engagement technologies can be utilized to deliver appointment reminders and for patient self-scheduling.
Postpartum care planning can be supported by the following technologies: clinical decision support, registries, care gap reports, screening data (BH, social needs, etc.), external referral reports and hospital delivery records. Equity data can be leveraged to identify patients at higher risk for postpartum complications.
Action steps and roles
These action steps were adapted from Postpartum Discharge Transition Change Package. Institute for Healthcare Improvement. 2022
Readiness
1. Develop and maintain a set of referral resources and communication pathways.
Suggested team member(s) responsible: Clinic manager and referral coordinator.
Referral and communication pathways between obstetric providers, hospitals, community-based organizations, and state and public health agencies can enhance access to and utilization of services and supports for pregnant and postpartum families.
Making referrals encompasses a spectrum of potential information-giving and supportive behaviors ranging from providing information on specific services to follow-up on service utilization and outcomes and assessment of the quality of referrals.[41] “Cold” and “warm” are often used to describe referral behaviors at two points along this spectrum.[42] A cold referral means providing information to the client about another agency or service, and it is then the client’s responsibility to contact the agency or service.[43] A warm referral involves contacting another agency or service provider on the client’s behalf. This entails calling and making an appointment for the client, providing support to overcome barriers to care, and following up to determine if the appointment has been kept.[44]
Agency policies should indicate the type of referral that is usually most appropriate for each service. Referral type may also depend on the client’s individual circumstances, so providers should use their best judgment.
Establish technology-based partnerships to allow staff at Community Health Centers (CHCs) to access hospital discharge summaries and other relevant inpatient records.
2. Ensure resource lists are available in languages representative of the populations in the health center service area.
Suggested team member(s) responsible: Translation staff.
Review resource lists to ensure availability in preferred languages spoken in the community and, when possible, refer patients to resources and services that are available in their preferred language.
3. Collaborate on the development of a patient-facing discharge summary form.
Suggested team member(s) responsible: Outpatient clinicians, prenatal assistants, hospital staff.
Wherever possible, postpartum appointments should be made prior to discharge from the birth facility for your patients. Discharge summaries can serve as a mechanism for patient and family member engagement and postpartum education. Convene an interdisciplinary team of inpatient and outpatient providers to develop a standard patient-facing discharge summary form that highlights risk factors, complications or diagnoses, necessary follow-up, and health system contact information. Engage people with lived experience in development of patient-facing discharge summary documents to ensure they are clear, understandable and meet patient needs.
4. Educate clinicians and staff on optimizing postpartum care.
Suggested team member(s) responsible: Medical director or designates, clinic manager.
Providing multidisciplinary staff education on optimizing postpartum care, including why and how to screen for life-threatening postpartum complications and how to engage family members and caregivers in discharge education and planning will ensure that any encounter birthing people and family members have with health center staff is an opportunity for prevention or early intervention.
The schedule of postpartum visits encourages the postpartum person to see their provider at three weeks, six weeks and 12 weeks after birth. It is important to remember that postpartum recovery can take approximately six months or longer. By engaging in whole-person care, health centers will engage the postpartum pen and their support network to ensure optimal health outcomes and any identified concerns can be mitigated.
5. Support professional development opportunities on trauma-informed practice and protocols.
Suggested team member(s) responsible: Medical director or designates.
Developing trauma-informed protocols and trainings to address healthcare team member biases enhances quality of care. See resource: Trauma-Informed Population Health Management)
6. Educate clinicians and staff on how to use a standardized discharge summary form.
Suggested team member(s) responsible: Informatics team, EHR IT.
Clinicians and staff ability to effectively review patient data ensures that recommendations made for postpartum care follow-up and community services and resources have been carried out. Health centers will review the mechanisms that are in place to share delivery and discharge information with obstetrician (OB) or midwife and primary care provider (PCP), with consideration for situations where the delivery hospital is not part of the same system as the OB, midwife or PCP.
Ensure clinicians and staff recognize that patients and family may be the primary source of information at the time of visit, if outside records are not available.
Recognition and prevention
7. Discuss reproductive desires during prenatal visits and revisit at postpartum visit.
Suggested team member(s) responsible: Providers and clinic staff.
Prenatal visits should include discussion about the birthing person’s reproductive desires, including the desire for and timing of any future pregnancies, and include in postpartum care plans. Offer appropriate resources, including access to a full range of contraceptive options in accordance with safe therapeutic regimens.[45] A birthing person’s future pregnancy intentions provide a context for shared decision-making regarding contraceptive options.
At the postpartum visit, re-assess previously stated contraception preferences and provide relevant services.
8. Provide anticipatory guidance during pregnancy with the development of a postpartum care plan that addresses the transition to parenthood and well-person care.
Suggested team member(s) responsible: Providers and clinic staff.
Providing anticipatory guidance during prenatal visits optimizes postpartum care and can help to inform the development of a postpartum care plan. Collaboratively design postpartum care plans that emphasize patient and family needs and wishes by engaging in open, transparent and empathic communication. Encourage the participation, as appropriate, of the support network in the development of a postpartum care plan.
The American College of Obstetricians and Gynecologists (ACOG) suggests components of the postpartum care plan include care team member names (inclusive of family and friends) and contact information; time, date and location of postpartum visits; infant feeding plan; reproductive life plan; pregnancy complications and follow-up; and anticipatory guidance regarding signs and symptoms of perinatal depression or anxiety. See ACOG Committee Opinion Number 736: Optimizing Postpartum Care. May 2018 for a complete list of suggested components for postpartum plans.
9. Establish a system for scheduling the postpartum care visit and needed immediate specialty care visit or contact (virtual or in-person visit) prior to discharge or within 24 hours of discharge.
Suggested team member(s) responsible: Clinic manager and prenatal assistants.
All postpartum people should have contact with a perinatal care provider within the first three weeks postpartum. This initial assessment should be followed up with ongoing care as needed, concluding with a comprehensive postpartum visit no later than 12 weeks after birth. The timing of these visits should be individualized and person-centered. Attempt to schedule the patient with their preferred perinatal care provider who they saw during their pregnancy.
10. For primary care or other non-OB/GYN settings, assess and document if a patient presenting is pregnant or has been pregnant within the past year.
Suggested team ”ember(s) responsible: Providers and clinic staff.
Include the question, "Have you been pregnant in the last year?" in standard intake scripts in EHR, and ensure gender inclusivity in assessment. If they answer yes, assess for need for prenatal or postpartum services. Screen for postpartum risk factors and provide linkage to community services and resources.
Response
11. Conduct a comprehensive postpartum visit for at least 30 minutes.
Suggested team member(s) responsible: Providers and clinic staff.
The comprehensive postpartum visit should include a full assessment of physical, social and psychological well-being.4 This is also an opportunity to engage the postpartum patient in discussions around elements of postpartum self-care. Consider scheduling needs to allocate sufficient time in the provider’s schedule.
12. Engage the birthing person’s support team.
Suggested team member(s) responsible: Providers, social workers, clinic staff.
Encourage the presence of a designated support person (e.g., doula, CHW, partner, friend, family member) during all instances of care as desired and particularly when teaching or education occurs. Connect the patient with local birth centers and peer support groups for additional community building and postpartum support, like lactation support or new parenting groups.
Reporting and systems learning
13. Develop and systematically utilize a standard comprehensive postpartum visit template.
Suggested team member(s) responsible: EHR IT, clinic manager, providers, clinic staff.
Engage a multidisciplinary team to create and test a standard postpartum visit template. Include patients in the development of the template to ensure the visit components meet their needs.
14. Identify and monitor postpartum quality measures.
Suggested team member(s) responsible: QI and implementation team.
Review all process and outcome data disaggregated by race, ethnicity and language to assess for inequities. Engage clinicians and staff in the review and discussion of the data. Engage leaders in messaging about destigmatizing discussion and identification of inequities to ensure diverse populations have access to respectful, whole-person, quality care. Include patient-facing surveys or other feedback options.
15. Monitor data related to completed postpartum comprehensive visits.
Suggested team member(s) responsible: QI and implementation team.
Disaggregate postpartum comprehensive visits by race and ethnicity, at a minimum, to evaluate disparities in rate of follow-up visit completion and identify strategies for improvement. Consider sharing data on postpartum visit attendance with hospital systems where patients deliver and identify strategies to improve referral and scheduling processes.
Respectful, equitable and supportive care
16. Include each pregnant or postpartum person and their identified support network as respected members of and contributors to the multidisciplinary care team.
Suggested team member(s) responsible: Providers and clinic staff.
By facilitating open conversations with the pregnant or postpartum person helps to ensure that concerns are adequately addressed, and there is opportunity to investigate possible causes when patients express that something is "off." Having a member or members of the birthing person’s support network present during these conversations may help to unearth concerns as well as ensure the appropriate support is in place when the patient returns home. During these conversations providers should consider ways in which implicit bias and structural racism may influence response to patient concerns and response to pain.
17. Promote life-long learning among clinicians and staff.
Suggested team member(s) responsible: Leadership team, including medical director and clinic manager
Educate clinicians and staff on providing respectful care by engaging in the lifelong learning of cultural humility, understanding that individuals cannot learn all aspects of any culture, including their own.
Review local resources and benefits available to pregnant and postpartum clients to increase staff and provider knowledge of such services. See more in Key Activity 17: Continue to Develop Referral Relationships and Pathways and Key Activity 18: Strengthening Community Partnerships.
FIGURE 15: POSTPARTUM VISIT TOPIC CHECKLIST
Checklist Domain |
Checklist Item |
|---|---|
General |
|
Postpartum problem list |
Pregnancy conditions requiring follow-up (e.g., anemia, GDM, latent TB, immunization status, depression). |
Vitals and physical exam |
|
Screenings |
|
Other topics |
|
Referrals, if indicated |
|
Evidence base for this activity
Alliance for Innovation on Maternal Health (AIM) Patient Safety Bundles: Postpartum Discharge Transition.
KEY ACTIVITY #10:
Support Patient Self-Care
This key activity involves the following elements of person-centered population-based care: proactive patient outreach and engagement; care coordination; behavioral health integration.
Overview
The term “self-care” refers to patients’ engagement in the activities and decisions that improve their health and well-being. Supporting self-care involves activities that enhance the capacity of individuals to engage in their care. Research demonstrates that pregnancy can be a particularly impactful time for patients to make positive changes with respect to self-care[46].
Why this matters
To address their healthcare needs, patients and families must have skills and knowledge to make healthy lifestyle choices. This is a daunting task, but perinatal care providers can help by taking opportunities to enhance the ability of patients to self-manage through provision of resources tailored to patient needs and providing the coaching in self-care practices.
Evidence suggests that supporting self-care can improve patient outcomes and quality of life.[47] In addition, a focus on the capacity of individuals in underserved segments of the population to engage in their care is foundational to ensuring equitable care delivery. Pregnant patients can utilize self-care approaches to support their own health and wellness as well as gain knowledge to advocate for themselves and their families.
Technology Considerations
This activity is supported through consideration of the wide and proliferating range of patient-facing applications and technologies. These also now include home patient monitoring devices. Given the challenges with equitable access to technology, a multimodal approach to support patients is important. The range of opportunities to provide patient support and education include face-to-face session, telephone session, asynchronous communication tools (e.g., patient portals and texting modalities) as well as telehealth visits.
For the pregnant population, numerous evidence-based apps are available for clients to use to track their pregnancies progress and learn about common discomforts. For pregnant patients with medical conditions like gestational diabetes, consider recommending apps to help monitor blood glucose levels and nutritional goals.
Relevant health information technology (HIT) capabilities to support this activity include electronic access to prenatal care guidelines, registries, clinical decision support, care dashboards and reports, quality reports, outreach and engagement, and care management and care coordination.
Action steps and roles
1. Improve information resources for patients.
Suggested team member(s) responsible: If a patient and family advisory council is in place, ask them to develop and/or refine patient information materials along with clinic staff.
- Update patient information materials, translating to language prevalent in the community, and reviewed by patients and families where possible.
- Support patient use of a patient portal that links to reputable health information. Consider including links to respected websites and social media accounts.
- Be aware of each patient’s health literacy, their ability to use health information effectively. Ensure materials are written at appropriate literacy level.
- Discuss a patient’s interest in information about health topics during clinic visits and preferred ways to receive information. Rather than assuming a patient needs and wants certain information, use tips from the field on motivational interviewing to ask open-ended questions.
Tip: Self-care coaching can begin with new patients. Consider holding on-boarding group visits for new pregnant patients that orient the patients to the clinic, its workflows and resources, and opportunities for self-care support.
2. Identify opportunities to enhance patient knowledge and confidence.
Suggested team member(s) responsible: Clinic staff including social workers, educators, nurses and providers.
Enhance knowledge and emotional support through a support network of family, friends and doulas so that the patient feels empowered to fully utilize health resources, services and supports.
Birth plans can be a particularly impactful way to engage clients in their own prenatal and birth experiences. ACOG and the California Maternal Quality Care Collaborative have resources to share with clients regarding birth plans.
3. Implement shared care plans with patients.
Suggested team member(s) responsible: Care team, patients and family members, if appropriate.
Shared care plans (see AHRQ Shared Care Plans) involve decisions of how the patient/provider discussion will be fit into the clinic visit workflow; training in facilitating collaborative conversations with patients; what format a shared care plan will take (a pa vs. electronic copy to be shared at the end of any interaction); and how the shared care plan will be documented.
4. Address health-related social needs that impact self-care.
Suggested team member(s) responsible: Care team.
- Implement universal Social Needs Screening and use the results to identify health-related social needs of patients. See Activity 7: Use Social Needs Screening to Inform Patient Treatment Plans for more information.
- Update a directory of community-based resources (see Activity 18: Strengthen Community Partnerships for examples) and routinely refer patients to appropriate resources through the care coordination process already in place.
- Follow up with patients who have been referred to community-based resources to learn if the referral was helpful.
- Begin self-care coaching in the exam room. Consider opportunities to leverage the extended members of the care team who often are representative of the populations you are serving. The self-management coaching can occur before being seen by a clinician (while waiting for the provider) and after seeing the provider. The key is to ensure the self-management coaching is well coordinated by the integrated care team.
- Self-care coaching for people with behavioral health conditions: National Institute of Mental Health (NIMH): Caring for Your Mental Health.
5. Implement self-management support.
Suggested team member(s) responsible: Care team.
- Self-Management Support (SMS) is a technique that enables patients to play an active role in their healthcare. SMS uses the ask-tell-ask approach, patient-directed goal setting, and follow-up to support individuals in making decisions that benefit their health and well-being. Training for staff and providers will be necessary to implement SMS.
- Assessment of self-activation capacity of patients can help health centers identify system-level interventions that can build self-care capacity at a population level. For example, offering classes for specific populations or group visits.
- See technology considerations for guidance on using apps to support self-care for pregnant patients.
Evidence base for this activity
Dineen-Griffin S, Garcia-Cardenas V, Williams K, Benrimoj SI. Helping patients help themselves: A systematic review of self-management support strategies in primary healthcare practice. PLoS One. 2019 Aug 1;14(8):e0220116. doi: 10.1371/journal.pone.0220116. PMID: 31369582; PMCID: PMC6675068.
Hibbard JH, Greene J. What the evidence shows about patient activation: better health outcomes and care experiences; fewer data on costs. Health Aff (Millwood). 2013 Feb;32(2):207-14. doi: 10.1377/hlthaff.2012.1061. PMID: 23381511.
Roy D, Meador M, Sasu N, Whelihan K, Lewis JH. Are Community Health Center Patients Interested in Self-Measured Blood Pressure Monitoring (SMBP) – And Can They Do It? Integrated Blood Pressure Control [Internet]. 2021 Feb [cited 2021 Aug 8];Volume 14:19–29. Available from: https://dx.doi.org/10.2147%2FIBPC.S285007.
Action of Patients for Successful Self-Management, J Ambulatory Care Manage Vol. 32, No. 1, Simmons, L., et al, 2009.
KEY ACTIVITY #11:
Behavioral Health Screening, Including Postpartum Depression
This key activity involves the following elements of person-centered population-based care: operationalize clinical guidelines; pre-visit planning and care gap reduction; behavioral health integration.
Overview
This key activity provides guidance on behavioral health screening during pregnancy and postpartum. All perinatal patients should be screened for mental health conditions. Prenatal and postpartum depression screening are both HEDIS supplemental measures. See the clinical practice guidelines for guidelines on prenatal and postpartum depression screening as minimum requirements. This recommendation aligns with ACOG’s Committee Opinions #757, “Screening for Perinatal Depression 1,” recommends screening patients at least once during the perinatal period for depression and anxiety, and, if screening in pregnancy, it should be done again postpartum. Practices who wish to go beyond the PHMI CGAG endorsed recommendations, consider Opinion #736, “Optimizing Postpartum Care 2,” recommends a full assessment of physical, social and psychological well-being within a comprehensive postpartum visit that occurs no later than 12 weeks after birth.[48]
The Substance Abuse and Mental Health Services Administration (SAMHSA) defines depression as a disorder of the brain. It is a serious mood disorder that is more than just a feeling of being "down in the dumps" or "blue" for a few days. Postpartum depression (PPD) affects gestational parents after having a baby. It causes intense, long-lasting feelings of anxiety, sadness and fatigue, making it difficult for parents to care for themselves and/or their babies, as well as handle daily responsibilities. PPD can start anywhere from weeks to months after childbirth. The American Academy of Pediatrics (AAP) recommends that pediatricians screen people who have given birth for PPD at the infant's one-, two-, four- and six-month well child visits.
Why this matters
Mental health conditions during pregnancy and the first year after childbirth are one of the most common conditions during pregnancy and postpartum, affecting more than one in five individuals.[49] [50] [51] Despite the existence of validated screening tools and effective, safe treatments, these conditions are often underdiagnosed and inadequately treated. Without intervention, fewer than 25% of individuals with perinatal depression will receive any treatment, and even fewer will receive adequate treatment or achieve remission.[52] [53] Early detection and treatment can alleviate negative consequences of these conditions and improve patients’ quality of life.
Leveraging this intervention to improve equitable health outcomes
According to The Institute for Diversity and Health Equity (IFDHE), part of the American Hospital Association (AHA), PPD affects one in eight people who have given birth; however, the risk is 1.6 times higher for Black people than white people. While the risk may be higher, Black people are less likely to receive help due to factors such as structural racism, a historical mistrust of the healthcare system, financial barriers, and stigma associated with mental health struggles. Perinatal mental health symptoms and issues among Black patients are often overlooked and under addressed. See Key Activity 4: Use a Systematic Approach to Decrease Inequities within the Population of Focus for additional guidance on addressing health disparities among pregnant patients.
Leveraging this intervention to attend to patients’ social needs
Comprehensive screening in physical, behavioral and social health domains is necessary to identify patients’ needs and wants across a whole-person spectrum of health. Treatment for depression in pregnancy and postpartum involves multiple modalities, including counseling, group therapy, and medication, that can be tailored to the patient’s individual needs.
Technology considerations
Technology can support screening for behavioral health conditions by delivering structured guidelines, protocols and clinical decision support to care team members responsible for carrying out assessments. It can also help by incorporating standardized screening tools into EHRs and care management and care coordination applications. These screening tools can also be made available directly to patients through patient outreach and screening technologies.
Understanding the prevalence of behavioral health conditions assists in program and resource development to track impact on health outcomes and to incorporate into risk stratification. Health information technologies used to track referrals are also important in care management.
Action steps and roles
Here is a sequence of steps that practices can use to implement screening for behavioral health conditions in the perinatal period.
1. Understand current recommendations for perinatal behavioral health screening.
Suggested team member(s) responsible: QI lead and frontline staff.
Current guidelines for screening are available as part of the Clinical Practice Guidelines for Key Medi-Cal Populations of Focus. Guidelines are also available from ACOG: Implementing Perinatal Mental Health Screening.
ACOG’s Clinical Practice Guideline 4: “Screening and Diagnosis of Mental Health Conditions During Pregnancy and Postpartum” recommends:
- Everyone receiving well-person, prepregnancy, prenatal and postpartum care be screened for depression and anxiety using standardized, validated instruments.
- Screening for perinatal depression and anxiety at the initial prenatal visit, later in pregnancy, and at postpartum visits.
- Implementing mental health screening with systems in place to ensure timely access to assessment and diagnosis, effective treatment, and appropriate monitoring and follow-up, based on severity.
- Completing screening for bipolar disorder before initiating pharmacotherapy for anxiety or depression, if not previously done.
- When someone affirmatively answers a self-harm or suicide question, clinicians immediately assess for likelihood, acuity and severity of risk of suicide attempt and then arrange for risk-tailored management.
- Clinicians provide immediate medical attention for postpartum psychosis.
2. Create a care gap report.
Suggested team member(s) responsible: QI lead and frontline staff.
Establish a baseline by assessing the percentage of patients or visits at which behavioral health screening occurred (e.g., postpartum depression screening was documented at 33% of visits at which postpartum depression screening is recommended to occur).
3. Flag all eligible patients for behavioral health screening and administer screening.
This should be programmed as an alert in the EHR so staff are aware at the time of visit.
There are many validated tools available. To screen for depression, consider:
- During pregnancy: Patient Health Questionnaire-2 (PHQ-2) and Patient Health Questionnaire-9 (PHQ-9) (PHQ-2 In Spanish; PHQ-9 in Spanish).
- During postpartum: Edinburgh Postnatal Depression Screen (EPDS). (In Spanish).
To screen for anxiety, consider:
- General Anxiety Disorder 7 (GAD-7) screen, seven questions.
To screen for posttraumatic stress disorder (PTSD), consider:
To screen for bipolar disorder, consider:
- Mood Disorder Questionnaire (MDQ), 14 questions. The MDQ needs to be done only once in the perinatal period as it queries lifetime experience as compared to the other screening tools, which ask how a person has felt in the last seven days to one month.
Combined tool:
4. Create a protocol to screen for behavioral health conditions.
Ensure standardized clinical workflows are in place for routine prenatal and postpartum screening. In many CHCs, medical assistants or other clinical support staff administer the mental health screenings in advance of the clinician visit. Clinicians then review the results and, if appropriate, offer relevant treatments or referrals.
To maximize completion of behavioral health and postpartum depression screening, the workflow should be executed at any visit where the new parent presents (e.g., at the first postpartum visit, integrated within the first well child visit with the pediatrician).
See the Perinatal Mental Health Conditions guide from Alliance for Innovation on Maternal Health.
5. Develop workflows for integrating postpartum mental healthcare, including provision of pharmacotherapy when indicated.
Identify mental health screening tools to be integrated universally in every clinical setting where patients may present.
- Establish an evidence-based, person-centered response protocol based on what is feasible for each area of practice and local mental health resources. Ideally, responses are tailored to condition severity and are strength based, culturally relevant and responsive to patient’s values and needs.
- Ensure staff can activate an immediate suicide risk assessment and response protocol as needed for patients with identified suicidal ideation, significant risk of harm to self and/or others, or psychosis.
- Include each pregnant and postpartum person and their identified support network as respected members of and contributors to the multidisciplinary care team.
- Provide information to prescribing providers and patients on evidence-based, safe pharmacological depression treatment options for pregnant and postpartum patients. ACOG has clinical practice guidelines outlining such medications.
6. Educate clinicians, frontline staff, administrative staff, patients and patients’ designated support networks on optimal care across the preconception and perinatal mental health pathway, including prevention, detection, assessment, treatment, monitoring, and follow-up best practices.
- Facilitate trauma-informed training and education to address healthcare team member biases and stigma related to mental health conditions, including anti-racism considerations.
- Incorporate mental health into multidisciplinary rounding to establish a non-judgmental culture of safety.
- Provide staff and provider training on common modalities to treat depression in pregnancy and postpartum.
- Engage in open, transparent, empathic and trauma-informed communication with pregnant and postpartum people and their identified support network to facilitate understanding of diagnoses, options and treatment plans.
7. Develop and maintain a set of referral resources and communication pathways between obstetric providers, community-based organizations, and state and public health agencies to address patient needs, including health-related social needs.
- Establish care pathways that facilitate coordination and follow-up among multiple providers throughout the perinatal period for pregnant and postpartum people referred to mental health treatment.
- Identify local resources for mental health conditions necessitating immediate treatment (e.g., postpartum psychosis, suicidality).
- Ensure clear protocol for communication between pediatric providers and OB/GYN and primary care providers when a parent has a positive screen at a well child visit.
- Incorporate resources that recognize the range of providers and services that can provide mental health support from community groups to licensed providers. Personalize referrals depending on the needs of the client.
- Therapists, psychiatrists, doulas, midwives, social workers and new parenting groups.
8. Screen and provide linkage to resources for structural and health-related social needs that may impact clinical recommendations for treatment plans.
- Transportation, childcare and housing, among other factors, may impact a patient’s ability to adhere to a mental health treatment plan.
Example of how this activity has been implemented
In one clinic, the quality manager and the clinic manager evaluated subsets of the data, including postpartum depression screening completion rates by age, gender, race, ethnicity and geographic location to narrow the focus of potential process improvement activities. The data demonstrated that pregnant Hispanic patients in three unique zip codes were 50% less likely to be screened for prenatal and postpartum depression as compared to other patients.
In response, clinic staff developed a focused outreach campaign for these patients. Educational materials were created in patients’ preferred languages to address frequently asked questions and concerns about depression and the need for depression screening, especially during the prenatal and postpartum periods. The MAs in the clinic – fluent in Spanish, the predominant language of the segmented population – conducted telephone outreach, discussing prenatal and postpartum depression, benefits and risks associated with not receiving screening, addressed questions, and helped patient schedule past due prenatal and postpartum care appointments.
One patient, Maria, had just delivered and brought in her newborn for their first well child visit. During her child’s visit, the practice MA had Maria complete a PHQ-9, and her score was 17 (moderately severe depression). The provider informed Maria’s PCP and initiated a referral for cognitive behavioral therapy. Maria’s PCP considered if an antidepressant medication was needed. The care manager created a care plan with Maria to include postpartum depression education and coaching on self-management. After 30 days, the care manager reviewed her patient panel and identified that Maria was due for a repeat PHQ-9. Outreach was initiated to get the patient scheduled for either an in-person or telehealth visit to follow up on how she was doing, and to complete an interval PHQ-9 to measure the effectiveness of care. Maria repeated a PHQ-9, and her score is still a 17 (still moderately severe depression). The care manager conducted a case review with the PCP and behavioral health clinician to discuss Maria’s treatment plan and initiate changes in treatment. Treatment changes, including a referral to a community-based peer support group for new moms, were reviewed with Maria, and the care plan was updated. Follow-up appointments were scheduled.
Resources
Prenatal and postpartum depression screening tools.
KEY ACTIVITY #12:
Proactively Reach Out to Patients Due for Care
This key activity involves the following elements of person-centered population-based care: operationalize clinical guidelines; pre-visit planning and care gap reduction; behavioral health integration.
Overview
This activity provides guidance on how to effectively outreach to patients due for care. Proactive outreach can ensure patients follow through on recommended care. This is particularly important during pregnancy and postpartum when recommended care and referrals often are time-sensitive.
As part of pre-visit planning (PVP) and other clinical workflows, your practice should conduct some level of outreach to provide patients with information they may need to prepare for upcoming visits or engage in follow-up care plans determined during the visit. In addition, most electronic health records (EHRs) can be integrated with an automated reminder system for upcoming appointments and for patients who appear to have gaps in care. Patient outreach also occurs as a part of Care coordination, especially around supporting patients to engage in external referrals and in follow-up to a hospital admission or discharge. See Key Activity 13: Coordinate Care for further guidance.
Proactive outreach focuses on identifying subpopulations among patients who may benefit from additional outreach and implementing more personalized reminders and “touches” for them to engage in care.
Outreach to people who are not yet actively engaged in care goes beyond this foundational activity. See the "Going Deeper” Key Activity 18: Strengthen Community Partnerships for more about identifying trusted messengers in your community
Why this matters
Proactive outreach supports patients to remain engaged in care. It provides an opportunity for health needs to be identified and for patients to connect to appropriate care in a timely manner. As untreated health needs can lead to worse outcomes, proactive outreach may improve health outcomes. In the context of prenatal care, proactive outreach can identify missed appointments with specialists, ultrasounds needing to be completed, lab results missing from a patient’s chart or patients who have been out of care for extended periods of time. Because there is often two to four weeks between clinical visits during pregnancy, outreach interventions can ensure timely completion of important prenatal care testing and imaging.
Leveraging this intervention to improve equitable health outcomes
Focus on equity by using data to identify which populations, subpopulations or groups the current outreach and education efforts don't reach. See the PHMI Data Quality and Reporting Guide for more information.
Collaboratively designing outreach strategies with community partners and current patients promotes cultural humility and sensitivity. Tailored outreach with personalized reminders addresses diverse needs, reducing disparities in access to care.
Leveraging this intervention to attend to patients’ social needs
Health-related social needs (e.g., income insecurity, transportation issues and health literacy) can result in no-shows and deterioration of patient health status. Proactive outreach, coupled with awareness of clues to health-related social needs, can connect patients to community resources and help to establish trust in the care team.
Technology considerations
This activity relies on similar capabilities as care gap management, utilizing population views and registries to track prenatal care gaps against screening guidelines. These registries can be utilized to generate outreach lists for appointment schedulers and/or care managers and other care team members who might be tasked with contacting patients due for services. Many EHRs are capable of storing next appointment data that can also be used to generate lists, and may link to automated appointment outreach workflows. Patient-facing outreach and engagement technologies can be utilized to deliver appointment reminders and for patient self-scheduling. Care managers might use care management applications to track and prompt prenatal care needs, as well as postpartum visits.
Action steps and roles
1. Identify subpopulations among your obstetric patients who may benefit from outreach.
Suggested team member(s) responsible: Panel manager or data analyst with care teams.
- Start with frequent no-show patients and seek to understand their root causes, which may be related to social health-related needs or health literacy issues.
- Ask your care teams to identify patients they consider high-risk patients who have been lost to care.
- Use care gap reports to identify patients who are behind on prenatal testing or imaging or who have missed multiple prenatal visits. Patients who are engaged in care may still need additional care coordination or support. See Key Activity 3: Use Care Gap Reports or Registries to Identify All Patients Eligible and Due for Care for further guidance.
2. Establish the outreach model for your practice.
Suggested team member(s) responsible: Practice leadership.
One outreach model commonly used is to hire dedicated staff as population health specialists. This person would be responsible for using care gap reports to conduct proactive outreach to patients and schedule needed follow-up. See more about this in the care team duties and recommended education resource.
However, different teams may adjust this role to fit their context. An alternative model ensures each care team includes staff with knowledge of the local environment and available resources. These team members conduct telephonic outreach to higher needs patients and their families.
Train all outreach staff in cultural humility, motivational interviewing skills, and in the use of trauma-informed care.
3. Supplement your reminder system for contacting various subpopulations.
Suggested team member(s) responsible: Population health specialist with guidance from implementation team and IT staff.
Reminders should be sent to all persons with an upcoming scheduled appointment. The clinic scheduling system will likely have a function for generating automated reminders with an option for patients to cancel or reschedule if they cannot keep the appointment. Reminders should also be sent to all patients who appear to have gaps in care and missed appointments. See more in Key Activity 3: Use Care Gap Reports or Registries to Identify all Patients Eligible and Due for Care about updating your care gap reports to enable setting up automated reminders.
Automated reminder systems can support efficiency and reliability. However, more intensive reminders where the patient receives a personalized telephone call from their care team may help patients who are at higher risks of nonattendance or being lost to care.[54]
FIGURE 16: PROACTIVE OUTREACH & ENGAGEMENT EXAMPLE
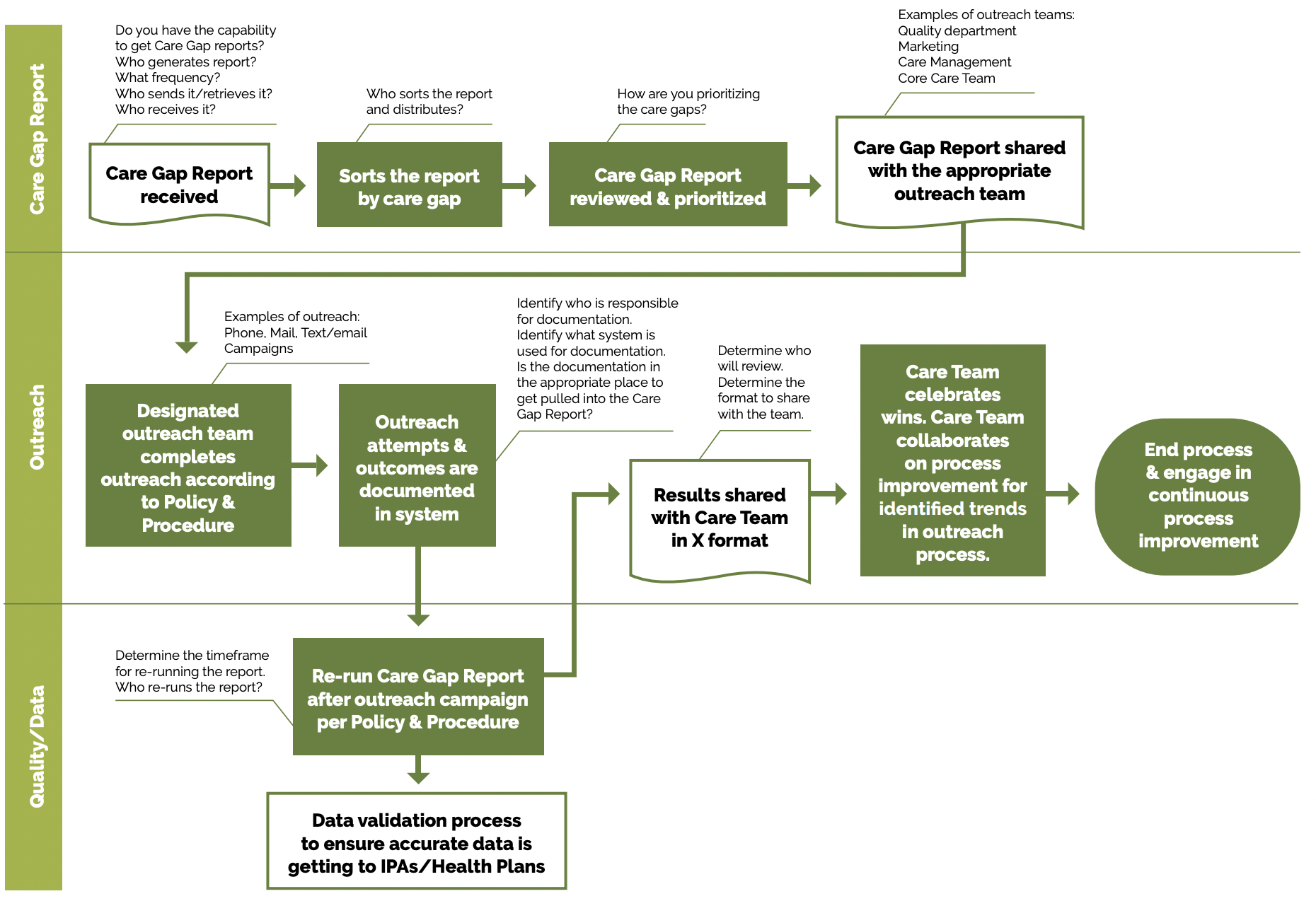
Utilize multiple pathways to reach and engage patients. For example, a Swiss clinic used sequential appointment reminders consisting first of a phone call and secondly of a text message if patients listed they received a postal reminder two days prior to their appointment. The reminder system significantly reduced the rate of missed appointments and allowed the clinic to reallocate 28% of the canceled appointments.[55]
Tip: Consider scheduling these outreached patients on days when you might experience a lower volume of activity in order to provide sufficient time for providers and staff to attend to the multiple patient needs that may be present.
Whether automated or manual, reminders should accommodate language requirements, as well as documented patient communication preferences (text, email, mail or phone). Reminders that include information beyond just the date, time and place may be more effective.[56] Consider including an orientation about what to expect and supporting clinical information.
4. Use “touches” that provide alternatives to the traditional office visit.
Suggested team member(s) responsible: Extended care team, including Enhanced Care Management (ECM), complex care management (CCM), community health workers, and population health specialist with guidance from implementation team.
Assess what types of interaction and care can be provided outside this setting, and collaborate with patients as part of initial care planning to understand their preferences for communication and care team interactions. Examples include, but are not limited to:
- Nursing visits (virtual).
- Pharmacy visits.
- Group prenatal care.
- Women, Infants and Children (WIC) program.
- Comprehensive Perinatal Support Services (CPSP).
- Black Infant Health (BIH).
- California Nurse-Family Partnership (NFP).
- Digital communication through emails, texts and patient portals.
- Newsletters focused on a specific condition.
- Social media that includes discussion groups relative to the management of conditions of focus.
- Home visits for high-risk, vulnerable or mobility-challenged patients.
- Other technological solutions, such as apps focused on patient conditions, which provide a vehicle for ongoing engagement.
5. Establish a process for engaging pregnant patients who have not yet been seen for prenatal care.
Suggested team member(s) responsible: Multidisciplinary implementation team.
It is important for practices to make a proactive plan to build capacity to accommodate pregnant-but-not-yet-seen patients in the clinic. Practices should develop strategies for outreach and engagement with these populations in order to shift them from not yet seen to fully engaged in prenatal care.
6. Continuously reassess outreach approaches with a goal of improvement.
Suggested team member(s) responsible: Population health specialist and ECM lead care managers.
- Test your collaboratively designed outreach approaches and measure the effectiveness of your approaches. Review data (e.g., missed appointments, numbers lost to follow up, etc.).
- Survey patients to obtain retrospective and prospective feedback on outreach efforts.
- Engage ECM lead care managers to provide feedback on outreach efforts.
- Regularly update outreach strategies based on community feedback and changing demographics.
Evidence base for this activity
Biola H, Deyo J, Hayes T, Small L, Chaplin J, Pak-Harvey E, Granger T, Jung L, Fitzgerald L, Crowder C, Patel B, Stillwell T, Eisenson H, Granger B. Reaching the Hard-to-Reach: Outcomes of the Severe Hypertension Outreach Intervention. Am J Prev Med. 2020 Nov;59(5):725-732. doi: 10.1016/j.amepre.2020.05.030. Epub 2020 Oct 1. PMID: 33011006.
Denberg TD, Myers BA, Eckel RH, McDermott MT, Dickinson WP, Lin CT. A patient outreach program between visits improves diabetes care: a pilot study. Int J Qual Health Care. 2009 Apr;21(2):130-6. doi: 10.1093/intqhc/mzn060. Epub 2008 Dec 24. PMID: 19109334.
McLean SM, Booth A, Gee M, Salway S, Cobb M, Bhanbhro S, Nancarrow SA. Appointment reminder systems are effective but not optimal: results of a systematic review and evidence synthesis employing realist principles. Patient Prefer Adherence. 2016 Apr 4;10:479-99. doi: 10.2147/PPA.S93046. PMID: 27110102; PMCID: PMC4831598.
KEY ACTIVITY #13:
Coordinate Care
This key activity involves the following elements of person-centered population-based care: proactive patient outreach and engagement; pre-visit planning and care gap reduction; care coordination; behavioral health integration; address social needs.
Overview
This activity will help you provide care that is patient-centered and coordinated across all internal and external providers involved with the patient.
What is care coordination?
Care coordination involves deliberately organizing patient care activities and sharing information among all participants concerned with a patient’s care to achieve safer processes and more effective outcomes.
Care coordination is an integral part of providing high-quality population-based care in an ambulatory care clinic. In your practice, care coordination happens daily as part of standard work and includes activities such as assisting patients with referrals, managing patient messages and receiving incoming information from outside care partners, including pharmacies, specialists, hospitals and community partners (e.g., schools, employers and community-based organizations). For perinatal patients, care coordination also involves intentional communication pathways between the Community Health Center (CHC) and hospital system responsible for intrapartum care.
Managing care across multiple settings is often a source of frustration and dissatisfaction for both patients and providers. Lack of coordinated care can result in both duplication of services and lack of completion of needed services. When care is not coordinated, decisions can be made without a complete picture of the patient’s needs and goals. Practices that have effective care coordination processes often employ “closed loop referrals” as a best practice.xxvii xxviii In a closed loop referral, a referring provider can track the status of the referral (completed or pending) as well as the outcome of the referral, including whether additional follow-up is needed. When closed loop referrals are implemented, both provider and patient satisfaction is enhanced.
Effective care coordination in primary care clinics
There are four fundamental concepts when thinking about care coordination activities within your practice:
- Accountability | A key to successful care coordination is accountability. Clinics and systems that excel at care coordination take ownership and assume responsibility for care coordination activities. Examples of care coordination processes include development of infrastructure for care coordination, identification of staff responsibilities, and relationship building with referral partners. Together, these actions create the ability to support referrals and transitions and track them to completion.
- Patient support | Referrals and transitions often raise questions for patients and families, and can be a source of anxiety. Not only do the logistics of a referral or transition create questions, but also patients and their families can experience anxiety regarding the outcome or purpose of a referral or transition. When a practice can dedicate staff time to addressing the needs of patients and families, referrals and transitions are most likely to accomplish intended goals.
- Relationships and supports | Referrals and transitions work best when all parties – patients, primary care providers, and consultants – agree on the purpose and importance of the referral and the roles that each will play in providing care.
- Connectivity | Build relationships and agreements among providers, including community agencies, that lead to shared expectations for communication and care. Connectivity includes developing referral relationships, accepting accountability and creating data flow.
In order to conceptualize how practices can coordinate with community-based agencies (housing, food, income support), hospitals and ERs, and specialists, refer to the visual depiction of the care coordination model by the Center for Accelerating Care Transformation (ACT Center).
Who is care coordination for?
Care coordination can benefit all patients in your practice, and care coordination processes, such as closed loop referrals, can be applicable to many practice activities (see examples in the table “Care Coordination Quality Improvement Strategy” below). Common areas where care coordination can be enhanced include specialty referrals, behavioral health referrals and connections to community resources such as WIC and paid family leave.
Care coordination activities can also identify patients who need a higher level of support through a care management program (see Key Activity 19: Provide Care Management). Care management differs from care coordination in that a patient consents to and works directly with a care manager to create a care plan that is shared with an extended care team. While a practice can decide whether it has the resources to provide higher level care management services, care coordination is a foundational activity of effective population health management.
Care coordination for Medi-Cal members
Patients with Medi-Cal have access to many resources that can support improved health outcomes and social needs. These Medi-Cal resources can be another opportunity to create care coordination processes in your practice; see Figure 17 for a partial list of Medi-Cal programs that involve care coordination. As of 2023, both doula care and community health worker (CHW) services are a benefit of the Medi-Cal program. Doulas provide evidence-based, culturally competent (racial, ethnic, linguistic) services aimed at preventing perinatal complications and improving health outcomes for birthing (see Key Activity 15: Doula Programs). The services of CHWs, also known as Promotores or Community Health Resources, can be highly effective in helping to connect patients to resources and educational materials that are community-based and aligned with a patient’s values, language and cultural needs to further health equity. The California Health Care Foundation offers an overview of the CHW program, including potential hurdles.
Medi-Cal patients with high medical, behavioral health and/or social needs may be eligible for Enhanced Care Management (ECM) and Community Supports (see “Going Deeper” Key Activity 19: Provide Care Management for more information on these programs).
There are also a number of Medi-Cal programs which provide services and support to Medi-Cal patients who qualify. Care coordination between the practice and these programs can result in more integrated care for eligible patients. Some examples include:
- California Children’s Services (CCS): Care coordination and support for eligible children with high levels of medical needs.
- Long-term services and supports (LTSS): These are available to support individuals in the community and include skilled nursing facility services, personal care services, self-directed personal assistance services, in-home supportive services, and home- and community-based services.
Figure 17: Examples of Medi-Cal Programs or Benefits that Involve Care Coordination
• Enhanced Care Management
• Community Supports
• Community Health Workers
• Doula
• Long term services and supports (LTSS)
• California Children’s Services (CCS)
Why this matters
Effective care coordination helps your practice to better meet the broad range of pregnant patients' needs and preferences. It helps ensure that each patient's needs and preferences are known and communicated at the right time to the right people, and that this information is used to guide the delivery of safe, appropriate and effective care.
Key outcomes of care coordination:
- Greater patient participation and satisfaction.
- Close gaps and address inequalities in access to care that exist.
- Improved quality outcomes and potential to leverage quality financial incentives.
- Decreased staff burnout and duplication of services (e.g., “Let the system do the work”).
Leveraging this intervention to attend to patients’ social needs and equity
Effective care coordination helps to reduce health disparities among different populations by better identifying and then working to address a broad range of patient needs. When care coordination is effective, the patient is at the center of care and the patient's cultural, social and health needs are incorporated into a plan of care. By identifying outside clinical (e.g., hospital care and specialist care) and social supports (e.g., housing assistance, transportation and food insecurity, etc.) and creating pathways for coordination, the practice promotes equity by facilitating access to these services for all patients who need them. As part of a care coordination strategy, practices should consider the a growing number of aggregator organizations (see resources section below) that partner with community-based programs and resources centered around addressing social needs such as housing, food and community. Many of these community-based programs are tailored for specific demographic groups and can support patients in meeting their needs in a culturally competent way.
Technology considerations
Technology can be used to streamline and enhance care coordination. Care coordination technology tools can support care coordination activities such as registry, clinical decision support, care gap reporting, and patient outreach engagement technology. See additional considerations under “Address Connectivity” below.
Practices can use a care coordination self-assessment tool, such as those referenced in the action steps below, to determine if additional technology support would be indicated.
Care coordination software: Clinical decision support
Many EHRs have care coordination modules, which can be used to develop assessments and care plans. Alternatively, care coordination modules can be add-ons to EHRs. Care coordination software can support assessment, referral and coordination pathways (clinical decision-making support). Using a care coordination software module, a practice can develop an assessment with questions regarding a patient’s social health needs. If answers are positive, the software can be configured to provide referral pathways and prompt care coordination activities. For example, if a pregnant patient answers “yes” to questions on food insecurity, the assessment can prompt referral to local resources such as WIC, food banks, meal programs and nutritional supports. The system can also prompt the staff to reassess progress at the next visit.
For more information, see Appendix D: Guidance on Technological Interventions.
Action steps and roles
The action steps and roles outlined below provide a framework for assessing current state, developing a strategy, implementing care coordination, and monitoring and learning as you progress.
1. Establish a call to action for care coordination.
Suggested team member(s) responsible: Medical lead, care coordination staff, QI staff.
To achieve effective care coordination, your practice needs to see yourself as a hub or center for coordination of patient care.
- While all providers within a patient’s support network need to collaborate, your practice should view itself as accountable for care coordination for empaneled patients and patients who have been assigned to your practice by their managed care plan.
- Identify a care coordination team who will be responsible for leading the evaluation, assessment and implementation of care coordination activities.
- Share with the care coordination team why care coordination is important.
- Some areas to address:
- What is care coordination?
- Why does care coordination benefit staff and patients?
- Review proposed framework (assess, develop strategy, implement, monitor) to develop the care coordination activity.
- Identify and share some initial projects directed at enhancing care coordination.
- Invite and engage staff and patients to provide input on how they think care coordination can be enhanced.
- Discuss how to best incorporate feedback from patients.
- Use feedback from this activity and incorporate it into assessment.
2. Assess your practice’s current state of care coordination activities.
Suggested team member(s) responsible: Panel manager and QI lead.
Begin by asking and answering the following questions:
- What does the practice hope to achieve by implementing interventions to change the care coordination process?
- Which patient needs are the responsibility of the practice to provide care coordination within the practice)?
- Which patient needs will need to be addressed through external referral and collaboration (care coordination with entities outside the practice)?
- What resources are needed to improve the current state (data, input from care team members, input from care partners such as hospitals, specialty, behavioral health and social needs)?
Gather stakeholder input:
- Conduct interviews or surveys with patients, community members, care and case managers, community support providers and community-based organizations that have referral pathways to Medi-Cal managed care plans (MCPs), such as Comprehensive Perinatal Services Program (CPSP), home visiting programs, etc. to understand their perspectives on current care coordination processes, challenges, and areas for improvement.
- Conduct interviews with your care team to understand their perspectives on current care coordination processes, challenges and areas for improvement.
Analyze existing systems and processes:
- Review existing care coordination protocols, technologies and resources utilized by health centers.
- Explore how technology is currently being used to support care coordination. Then, explore how technology could be harnessed to streamline care coordination, improve data sharing, and/or enhance communication among providers.
- Review existing formal and informal linkage agreements.
- Conduct an analysis to determine patient needs not yet fully addressed by existing agreements.
- Assess data on patient outcomes including process outcomes (e.g., obtaining labs and imaging as recommended by providers; adherence to recommend prenatal and postpartum follow-up visits); clinical outcomes (e.g., reduction in C-sections, etc.); utilization outcomes (e.g., reduction in ED visits and hospitalizations); satisfaction; and any existing quality improvement initiatives.
- The following resources can help your practice assess its current state:
- Population Health Management Capabilities Assessment Tool (PhmCAT): Sections on population-based care, social health and behavioral health.
- Care Coordination Maturity Assessment: This resource addresses multiple domains that may be impacted as care coordination activities are undertaken.
3. Develop and implement a care coordination improvement strategy.
Suggested team member(s) responsible: Panel manager and QI lead.
Develop your high-level care coordination improvement strategy.
- The high-level strategy is based on the results and insights from your care coordination assessment and your practice’s capacity (bandwidth).
- Establish clear objective.
- Define specific, measurable, achievable, relevant, time-bound, inclusive, and equitable (SMARTIE) goals for enhancing care coordination.
- Ensure that these goals align with the overall mission and values of your practice.
- Prioritize areas for improvement. Identify a limited set of key focus areas, such as communication protocols, technology integration, staff training or patient engagement strategies, based on the assessment findings and your practice’s bandwidth.
Identify resources and infrastructure.
- As part of the implementation of the strategy, identify the resources and infrastructure needed to support care coordination at your practice.
- We have included in Figure 18 below some considerations by resource as you develop your care coordination implementation plan. Some of the resources may not apply to your practice.
FIGURE 18: CONSIDERATIONS FOR IDENTIFYING CARE COORDINATION (CC) RESOURCES
Resource |
Considerations |
|---|---|
Staff |
Dedicated time for the development, training and implementation of CC activity. Defining ongoing staffing needs. |
Internal tools |
Electronic health record modifications. Data needs and technology needed to implement CC activity. |
Process |
Development of workflows, training materials, communication plan and job descriptions. Identification of what CC activities will be the responsibility of the practice staff. |
Funding and finance |
Explore benefits (such as Enhanced Care Management or community health workers) as well as financial resources that may be available through external partners, such as health plans and hospitals. |
Clinical decision-making support |
Medical staff, behavioral health and social workers, and patients as subject matter experts (SMEs). |
External support and data |
Information and resources required from the entity with which the clinic is coordinating (e.g., hospital, specialist, social health provider). Data exchange requirements including the new California Data Exchange Framework (DxF). |
Develop staffing for care coordination.
- Determine who at your practice will be involved in care coordination. For many organizations, staff involved in the Comprehensive Perinatal Services Program will be key contributors, including ECM lead care managers, particularly the ECM birth equity population of focus.
- The PHMI Care Team and Workforce Guide provides an overview on care coordination using a care coordinator or referral manager.
- Based on the population of focus and the intervention, develop staffing requirements and any job description changes to embed care coordination into your practice.
- The responsibilities of a person or people fulfilling care coordination roles should include, at a minimum:
- Manage the referral process.
- Assist patients with transitions, such as those to and from hospitals and other institutions.
- Help patients resolve logistical, financial and/or other barriers to a successful referral.
- Link patients with community resources.
- Follow up with patients within a few days of an emergency room visit, hospital discharge or discharge from a treatment facility. This process should include the transitional care services (TCS) lead care manager during transitions of care.
- Ensure the safe transfer of patient data.
- Track progress (e.g., referral milestones).
- Assist patients who are having difficulties.
- Schedule follow-up and specialty appointments for and with patients.
- Formalize this role through a job description or position description.
- Provide regular training and support to care coordinator or referral coordinator or similar.
Develop or refine your policies and procedures for care coordination. At a minimum, include all of the following:
- Identifying patients who are eligible for care coordination.
- Defining the activities that are associated with care coordination (e.g., outreach, engagement, assessment and desired outcome).
- Managing the referral process.
- Ensuring the safe and timely transfer of patient data.
- Tracking progress through closed loop referral (see referral milestones above).
- Identifying patients who would benefit from higher levels of care coordination, such as care management interventions like complex and Enhanced Care Management (ECM) (see Key Activity 19: Provide Care Management).
Develop or refine your referral protocols.
- Develop clear guidelines for when and how to make clinical referrals.
- Include criteria for urgent versus nonurgent referrals.
- For each provider your practice will be referring to:
- Identify the information, format and process the provider requires to receive a referral.
- Share the information you will need back from the provider when the referral has been successfully made and/or once the service or support has been provided to ensure continuity of care and nonduplication of services.
- Formalizing this through a written agreement or compact is a good way to ensure expectations on both sides of a referral are understood.
- In working with community agencies or organizations that provide social support, the specific information that can and should be shared will depend on the service. It is important to have a mutual understanding about that information, using a written agreement where possible. At minimum, if the referral did not include a warm handoff, there should be an expectation that the practice hears back from the organization to let them know whether the patient followed up on the referral. Sample primary care checklist suggestions for assessing referral process.
Address connectivity. For any providers, patients, family and caregivers who you are exchanging patient data with, your practice should develop formal agreements and processes. Here are some considerations to facilitate information sharing among providers involved in an individual’s care.
- Integrate documentation platforms where possible and standardize how documentation is included in patient records.
- Ensure that behavioral health records are integrated into the overall EHR system to the extent permitted by law.
- Enable providers to access comprehensive patient information.
- Identify and assess participation in health information exchanges and/or social health information exchange systems where feasible to facilitate seamless sharing of patient information between clinicians. These exist in some communities and will develop over time. This explainer series from the California Health Care Foundation describes the new statewide health information exchange coming into effect in 2024.
- Understand when patient consent is required to ensure compliance with privacy regulations, such as the Health Insurance Portability and Accountability Act (HIPAA). Include consent processes in the referral protocols.
o Set expectations about the information that should be shared and develop processes for facilitating that exchange. As data that is used in a clinical setting will likely be different than information that is shared by community agencies or social support networks, it is imperative to have clear parameters around what types of information can be exchanged between your practice and your partners.
Provide care coordination to patients.
- Provide care coordination to patients who need it in accordance with your care coordination policies and procedures and referral protocols.
- Embed care coordination into your practices daily workflow, including pre-visit planning. See Key Activity 6: Develop or Refine and Implement a Pre-Visit Planning Process.
- Provide referrals to care management as discussed in Key Activity 19: Provide Care Management, such as ECM for patients who require more intensive support.
- Discuss each referral with the patient to ensure the patient understands the reason for the referral.
FIGURE 19: EXAMPLE OF A CARE COORDINATION QUALITY IMPROVEMENT STRATEGY
Area of Improvement |
Goal |
Why It is Important |
|---|---|---|
Development of registries and processes to outreach to pregnant patients who have not engaged in care. |
Bring individuals into prenatal care by the end of the first trimester. |
Early engagement in prenatal care is important for the wellness of both the pregnant person and fetus. |
Develop system to provide key patient information to hospital system by 36 weeks of gestation. |
Ensure hospital’s OB providers have access to essential patient information at time of delivery. |
Access to health conditions, completed testing and imaging, and risk factors improves intrapartum care and decreases redundancies. |
Development of a closed loop referral pathway for social services when social health barriers are identified. |
To support patients in receiving services that will be beneficial to addressing social health barriers, including those that are culturally aligned and based in communities where they live. |
Health outcomes, including health equity and access are improved when social health needs are met. |
Development of a perinatal referral pathway to specialty providers and the creation of a pathway to receive consult results. |
To optimize access to specialty services, including urgent referral and to ensure consultation results are available to OB providers. |
To ensure timely access for services, including urgent referrals. Receipt of consult information saves time and prevents duplication of services. |
Development of a process to follow up with patients after transitions of care, post hospitalization, and post-emergency department visit. |
To support optimal outcomes for patients post hospitalization and decrease the chance of rehospitalization. |
Transition from the inpatient hospital setting back to home often results in poor care coordination, which can lead to medication errors, repeated or incomplete diagnostic workup, and lack of clarity regarding what a patient needs post hospitalization. For additional details on transitional care services (TCS) for Medi-Cal managed care plan members, please refer to the PHM Policy Guide on Page 29. For the purposes of TCS, all pregnant and postpartum individuals are considered high-risk for TCS and have access to a TCS lead care manager. Please engage the TCS lead care manager in care coordination. |
The following resource can help your practice develop your care coordination improvement strategy:
4. Monitor continuous quality improvement of care coordination.
Suggested team member(s) responsible: QI lead.
- Develop both formal and informal mechanisms to obtain feedback from providers, staff and patients on the effectiveness of your practice’s care coordination efforts and to identify areas for improvement.
- Establish key performance indicators related to care coordination. Consider using the Agency for Healthcare Research and Quality (AHQR)’s Care Coordination Quality Measures in Primary Care (CCQM-PC). Your performance indicators will vary based upon your improvement strategy and the needs of patients, but may include metrics, such as:
- Number of pregnant patients engaged in care.
- Number of pregnant patients with GDM who have adequately controlled blood glucose.
- Percent of closed loop referrals by referral entity. Monitor and analyze metrics to gauge the effectiveness of your internal systems and how well each referral partner is promoting coordination and collaboration.
- Continue to build relationships with providers and community support agencies that are available to provide services to CHC patients.
- Consider developing and using a care coordination variance report. Here is a sample patient care coordination variance report.
Implementation tips
- An interoperable referral management system can help practices streamline the intake process, communicate with other providers and social service agencies, track the status and outcomes of referrals, and ensure that patients receive the appropriate level of care and support.
- Leverage community health information exchanges (HIE) or Cal HHS Data Exchange Framework Data Sharing Agreement to gain access to admission, discharge, and transfer information. Absent being able to access an HIE, establish relationships with your local hospitals to be able to gain daily notification of your patients being discharged.
Resources
CDPH dashboards
Resources on American Indian health programs and American Indian Maternal Social Support (AIMSS) program, Black Infant Health (BIH) and Pacific Islander maternal programs to support these groups facing high rates of maternal morbidity and mortality.
Additional CDPH Resources:
Going Deeper Key Activities
More advanced activities that build off of the foundational activities and that help ensure your practice can achieve equitable improvement in your prenatal and postpartum care.
KEY ACTIVITY #14:
Group Prenatal Care, Including Centering Pregnancy
This key activity involves the following elements of person-centered population-based care: care coordination; address social needs.
Overview
Group care models are particularly well suited to prenatal patients, given their focus on anticipatory guidance and creating spaces for peer support. Bringing patients with similar needs together for healthcare encounters increases the time available for the educational component of the encounter, improves efficiency, and reduces repetition. Group prenatal care has been shown to improve peer support, provider satisfaction and patient outcomes. Group prenatal care also can be cost-effective for CHCs and health systems.[57] It is important that, when considering the implementation of group prenatal care, your practice maintains the capacity to address individual patient needs and complications that might arise in the group but will then warrant one-on-one attention.
CenteringPregnancy (CP) is a group prenatal care model in which facilitators lead a cohort of eight to ten pregnant people of similar gestational age through a series of ten interactive group visits lasting 90 to 120 minutes each. Sessions driven by Centering’s curriculum cover medical and nonmedical aspects of pregnancy, including nutrition, common discomforts, stress management, labor and delivery, breastfeeding, and infant care. It is a promising prenatal care model that a growing body of evidence suggests can improve birth outcomes, improve rates of postpartum visit completion, and increase satisfaction with prenatal care. Research conducted so far suggests that CP holds promise especially for supporting improved birth outcomes for specific populations at highest risk for preterm birth, infant mortality, and other adverse health outcomes. In particular, studies have found that it reduced the risk of preterm birth for Black and African American individuals and their babies, supporting the value of the model as an option for this population.
There are over 40 CenteringPregnancy and related group prenatal care models in California. CP presents an opportunity to better engage patients in their prenatal care and to create welcoming clinical spaces for populations at increased risk of poor birth outcomes. For more information on CP, visit the Centering Healthcare Institute.
Why this matters
Evidence suggests patients who participate in group prenatal care have better prenatal knowledge, feel more ready for labor and delivery, are more satisfied with care, and initiate breastfeeding more often. There is no evidence that suggests that group prenatal care causes harm. Group prenatal care models are designed to improve patient education and include opportunities for social support while maintaining the standard risk screenings and physical assessments of individual prenatal care. Studies appear to demonstrate obstetric outcomes that are at least equivalent to individual prenatal care and even improved for some populations.
Concerns regarding increasing healthcare costs, healthcare provider availability, dissatisfaction with wait times, and the minimal opportunity for education and support associated with the individual care model have given rise to interest in group prenatal care.
Action steps and roles
1. Review group prenatal care interventions to identify which model may be appropriate for your practice and the populations it serves.
Suggested team member(s) responsible: Practice leadership, care team, financial lead, billers and coders.
There are several group prenatal models available including CenteringPregnancy. Learn about the models through research and by speaking with other health centers or organizations that are conducting group prenatal care as well as reaching out directly to the model developer. Remember that there will be costs associated with training and certifying your practice, depending upon the group prenatal care model you select to implement.
2. Assess the health center’s capacity to implement a group prenatal care model.
For the assessment, consider patient panel, provider capacity, physical space available to convene the groups, and clinicians and staff who would serve on an implementation team. Some prenatal group models have assessments that health centers and organizations can complete to guide this decision-making process. In the event that your health center does not have the capacity, consider researching available group prenatal care programs in your service area and community to refer clients to.
Determine if an opt-in or opt-out approach would be utilized for group prenatal groups enrollment. Consider whether some group visits can be conducted virtually.
3. Develop and maintain a set of referral resources and communication pathways.
Referral and communication pathways between obstetric providers, community-based organizations, and state and public health agencies can enhance access to, and utilization of, services and supports for pregnant and postpartum families.
Making referrals encompasses a spectrum of potential information-giving and supportive behaviors ranging from providing information on specific services to follow-up on service utilization and outcomes and assessment of the quality of referrals.[58] “Cold” and “warm” are often used to describe referral behaviors at two points along this spectrum.[59] A cold referral means providing information to the client about another agency or service, and it is then the client’s responsibility to contact the agency or service.[60] A warm referral involves contacting another agency or service provider on the client’s behalf. This entails calling and making an appointment for the client, providing support to overcome barriers to care, and following up to determine if the appointment has been kept.[61]
4. Ensure resources are available in languages representative of the populations in the health center’s service area.
Review resource lists to ensure availability in preferred languages spoken in the community, and when possible, refer patients to resources and services that are available in their preferred language.
5. Educate clinicians and staff on group prenatal care.
Educate health center staff on the value of group prenatal care and how it will be integrated into health center care services. Ensure providers and staff have the necessary information and materials to make referrals to group prenatal care. Some group prenatal care models (e.g., CenteringPregnancy) may charge for staff training and site certification.
6. Ensure a core implementation team is available to support group prenatal care.
Establish a core implementation team with dedicated time to implement group prenatal care with fidelity. Ensure facilitators receive necessary training to create a trauma-informed and culturally responsive environment.
7. Conduct continuous quality improvement.
Solicit feedback from individuals who participated in group visits to identify opportunities for program improvement and ensure that the intervention is culturally responsive and trauma-informed. Convene group facilitators and educators for check-ins and sharing of lessons learned and strategies for engagement and group facilitation.
Implementation tips
Specific group prenatal care models can be challenging to initiate and maintain. The cost of initiating some group prenatal care models in current obstetric practices may be a barrier to implementation. Take time to research options and ensure leadership buy-in to implement and sustain group care.
Resources
KEY ACTIVITY #15:
Doula Programs
This key activity involves the following elements of person-centered population-based care: operationalize clinical guidelines; implement condition-specific registries; proactive patient outreach and engagement; pre-visit planning and care gap reduction; care coordination; behavioral health integration; address social needs.
Overview
The Department of Healthcare Services (DHCS) added doula services to the list of preventive services covered under the Medi-Cal program in January 2023. Doulas are birth workers who provide health education, advocacy, and physical, emotional, and nonmedical support for pregnant and postpartum persons before, during and after childbirth, including support during miscarriage, stillbirth and abortion. Doulas are not licensed and they do not require supervision. Doulas also offer various types of support, including health navigation, lactation support, development of a birth plan, and linkages to community-based resources.[62] Pursuant to federal regulations, doula services must be recommended by a physician or other licensed practitioner. In November 2023, DHCS provided a standing recommendation for doula services covering the standard package of doula visits (nine total prenatal and/or postpartum visits and labor support) for all eligible beneficiaries across the state.[63]
Doula services will be available in fee-for-service Medi-Cal and through Medi-Cal managed care plans. Beneficiaries in a Medi-Cal managed care plan will receive doula services from their plan. Your practice can find doulas participating in Medi-Cal in your area using the DHCS directory. These doulas may accept patient referrals from your practice.
Why this matters
Doulas support pregnant individuals and their families with education and advocacy. Doulas, when welcomed into your practice, can be a valuable part of the patient’s care team. As described below, studies in diverse populations have demonstrated that clients who use doula services during pregnancy and the postpartum period experience a variety of positive health outcomes.[64] Encouraging your staff to learn about doula services and doulas practicing in your area can improve the quality of care your practice provides.
Leveraging this intervention to improve equitable health outcomes
Doula programs help address equity when they serve clients and families who are at greater risk of poor birth outcomes, often due to historical marginalization. In these circumstances, doulas – particularly doulas who are culturally concordant to their clients – have been shown to:
- Reduce the perceived negative impact of interpersonal and institutional racism by birthing people of color.
- Improve rates of participation in medical, prenatal and postpartum care visits.
- Improve rates of breastfeeding initiation and continuation among clients.
- Decrease rates of cesarean birth.
- Decrease the use of pain medication during labor.
- Lower self-reported symptoms of depression and anxiety postpartum.
Leveraging this intervention to attend to patients’ social needs
Doula programs address social health by:
- Helping pregnant individuals navigate the healthcare system and advocate for their needs and preferences.
- Providing culturally appropriate and person-centered care that respects the diversity and dignity of each individual.
- Enhancing social support and reducing isolation for pregnant people.
- Empowering pregnant and birthing people to take charge of their own healthcare needs beyond the perinatal period.[65] [66] [67] [68] [69]
Action steps and roles
1. Ensure your staff and providers are trained on doula scope of work and are connected to doulas who may be serving Medi-Cal beneficiaries in your area.
This may involve using the DHCS doula directory, reaching out to Medi-Cal managed care plans, and connecting with community-based organizations in your area who might be knowledgeable about local doula networks.
2. Revise practice policies to welcome doulas to accompany patients to their prenatal visits.
Implement best practices to integrate doulas into the care team (this tool kit may serve as a guide).
3. Proactively identify patients in your practice who are eligible to receive doula services and screen them for interest.
A Medi-Cal enrollee who is pregnant, or was pregnant in the past year, and either would benefit from doula services or requests doula services. To receive doula services, Medi-Cal enrollees must have a written recommendation from a physician or other licensed practitioner of the healing arts acting within their scope of practice (the existing standing recommendation from DHCS will suffice). Doula services are preventive services, and a written recommendation approves the following:
- One initial visit.
- Up to eight additional visits, which may be provided in any combination of prenatal and postpartum visits.
- Support during labor and delivery (including labor and delivery resulting in a stillbirth).
- Up to two extended, three-hour postpartum visits after the end of a pregnancy.
Create a workflow to refer interested patients to local doula providers, and provide recommendations for doula services in alignment with Medi-Cal requirements.
4. Find more information visit Doula Services as a Medi-Cal Benefit via DHCS.
Evidence base for this activity
Knocke K, Chappel A, Sugar S, De Lew N, Sommers B. December 2022 ISSUE BRIEF 1 Doula Care and Maternal Health: An Evidence Review [Internet]. 2022 Dec. Available from: https://aspe.hhs.gov/sites/default/files/documents/dfcd768f1caf6fabf3d281f762e8d068/ASPE-Doula-Issue-Brief-12-13-22.pdf.
KEY ACTIVITY #16:
Vaccines
This key activity involves the following elements of person-centered population-based care: operationalize clinical guidelines; implement condition-specific registries; proactive patient outreach and engagement; pre-visit planning and care gap reduction; care coordination; behavioral health integration; address social needs.
Overview
Immunization is a core part of primary preventive care for adolescents and adults; pregnant people are no exception. Several vaccinations are recommended during pregnancy and lactation[70]; this section will focus on two key vaccines of importance during pregnancy: influenza (“flu”) and tetanus, diphtheria, acellular pertussis (“Tdap”).
While this section focuses on flu and Tdap, there are additional new vaccine recommendations during pregnancy. If your practice already has high rates of patient receipt of flu/Tdap, you could consider implementing a project to improve uptake of vaccines against COVID-19[71] with seasonal or annual administration or respiratory syncytial virus (RSV) with administration once between 32 and 36 weeks of gestation.[72]
Why this matters
The flu and Tdap vaccines have well established health benefits for both pregnant individuals and their newborn infants. Pregnant individuals are at increased risk of severe illness from influenza as compared to the general adult population. Seasonal vaccination during pregnancy at any gestational age can prevent hospitalization and other severe complications of flu. Tdap vaccination during pregnancy, ideally between 27 and 36 weeks of gestation, has health benefits for newborns, who receive passive immunity to protect them from whooping cough until they can begin pediatric immunizations against these infections at two months of life.
The receipt of flu and Tdap vaccines among pregnant patients is also of growing interest as a care quality measure. Both are recognized by the National Committee for Quality Assurance (NCQA)[73] [74] as key adult preventive care quality measures. Immunizations are also a good focus for quality improvement projects; the intervention is rapid and measurable with a clear eligible population. Improvement projects in this area are recommended by the Centers for Disease Control and Prevention (CDC) and others.
Leveraging this intervention to improve equitable health outcomes
Disparities in vaccine uptake can magnify existing inequitable health outcomes seen in the perinatal population. A prime example of this relationship was seen during the COVID-19 pandemic. Rates of vaccine uptake were lowest in those groups[75] – racial and ethnic, income-level, employment type – who were also at greatest risk of severe COVID-19 disease or death in pregnancy.[76] While the disparities in maternal and infant health outcomes seen in California are multifactorial, immunization equity can play a role in improvement.
A quality improvement project focused on certain subgroups less likely to be offered or accept the flu and/or Tdap vaccines during pregnancy could also mitigate inequities in your patient population. Studies[77] [78] have demonstrated racial disparities in flu/Tdap immunization uptake during pregnancy; some of these studies show that a provider recommendation can promote vaccine receipt in these groups.
Leveraging this intervention to attend to patients’ social needs
While patient-level hesitancy may be one factor playing into an individual’s decision to accept a recommended immunization, a variety of health-related social needs can combine to play an even greater part in this choice.
Measures of economic and social deprivation are known to be linked with rates of vaccine coverage among adults and children. Addressing health-related social needs in your practice can improve vaccination rates – a lesson learned during the COVID-19 pandemic).[79] For example, providing transportation resources, extended appointment hours (to account for inflexible jobs and school), walk-in vaccine clinics, and educational materials that are literacy level and language appropriate may have a positive impact.
Using data on the needs of your patient communities may help you focus your immunization improvement project on a population that could use more support. The California Healthy Places Index[80] may provide you with relevant information to guide project development.
Action steps and roles
1. Evaluate vaccine uptake data.
Suggested team member(s) responsible: Clinical lead and data lead.
Perform a chart review to identify rates of uptake of flu and Tdap vaccine during the appropriate prenatal windows. You can also leverage external validated sources of immunization data (e.g., California’s state registry). Linking your EHR to state registry data will allow your staff access to a patient’s full immunization record. In addition, you can leverage this data to get an accurate picture of your quality performance.
Beginning to analyze these data will allow you to answer important questions to design your improvement project. Is performance better in one vaccine than the other? Are certain patient subpopulations less likely to be vaccinated (use REAL/SOGI data)? Knowing what your baseline data look like will also help you to set performance improvement goals.
2. Assess practice infrastructure to support vaccine administration.
Suggested team member(s) responsible: Operations lead and clinical support staff.
While providing onsite immunizations may be standard practice in a pediatrics office, it may not be an existing perinatal care service in your office. Ensure that you have the correct procedures in place to provide vaccines at the point of care (associated with higher levels of acceptance). This may include: cold storage and monitoring, ordering and forecasting demand, supply chain development, and training on new staff policies and procedures.
3. Billing for vaccine administration (adults).
Suggested team member(s) responsible: Operations lead, finance lead, providers.
If providing onsite vaccinations is new to your perinatal practice, ensure that the appropriate billing and coding procedures are in place. This may help you track improvement data and will support the financial sustainability of your new service.
4. Engage the whole practice team in promoting vaccine uptake.
Suggested team member(s) responsible: Entire practice team.
Your practice’s administrative staff and clinicians should all share the same positive message about vaccine uptake during pregnancy. Ensure all members of the team have accurate information to share with patients regarding the benefits of vaccine administration on patient and newborn health. Your nonclinical partners (CHWs, doulas, peer support persons), ECM or complex care management (CCM), and transitional care services care managers may be particularly effective trusted messengers on vaccine benefits to your patient community.
5. Create educational materials to support informed decision-making regarding vaccines.
Suggested team member(s) responsible: Clinical lead, nonclinician partners, community-based organization partners, patients.
Educational materials for patients on the benefits and risks of accepting the flu and Tdap vaccines during pregnancy can support informed decision-making about this preventive service. Clinical team members can be sure the information provided is accurate; materials should be translated into relevant languages and written at an appropriate reading level. Nonclinician partners, community organizations and patients can review materials to ensure they speak to true patient concerns.
6. Think creatively about addressing health-related social needs that are barriers to vaccine acceptance.
Suggested team member(s) responsible: Entire team, nonclinician partners, community partners, patients.
Look to your community partners and patients for suggestions on what some nonmedical barriers might be. Should your practice arrange transportation vouchers for immunization appointments? Could you put on a mobile vaccine event (e.g., seasonal flu) in community spaces where pregnant patients already gather?
Implementation tips
These resources may help you in designing and implementing your practice’s immunization improvement activities.
- CDC-recommended adult vaccination schedule
- Patient education resources on vaccination in pregnancy (March of Dimes)
- California Healthy Places Index
KEY ACTIVITY #17:
Continue to Develop Referral Relationships and Pathways
This key activity involves the following elements of person-centered population-based care: operationalize clinical guidelines; pre-visit planning and care gap reduction; care coordination; behavioral health integration; address social needs.
Overview
Delivery of quality perinatal care encompasses not only clinic and hospital-based obstetric services, preventative care services, and coordination of medical and behavioral healthcare but also referrals for specialty care, social supports, dental care, and other needs of patients, such as birth classes or parenting programs. As a result, coordination of care is more complex and often involves referrals outside the practice structure. Examples include referrals from the practice to a provider (e.g., maternal fetal medicine specialty providers) as well as referrals to behavioral health and social services providers (e.g., WIC, CalFRESH, and CalEarn). A referral network also includes acute and subacute facilities, such as hospitals, emergency departments and residential treatment facilities where a patient may receive treatment and the outcome of treatment is necessary for the ongoing care of the patient in the practice.
This activity addresses common steps that your practice can take to optimize both the referral pathways and outcomes. Prioritize the practice of “ closed loop referrals” in which there is a feedback mechanism to ensure that a referral made by one provider to another is completed and followed up appropriately; “closed loop referrals” leads to greater patient and provider satisfaction. This activity builds on an inventory of existing referral services outside the clinic and identifies steps that can be taken to support the systematic management of the referral process.
Why this matters
When a patient requires a referral to obtain needed services outside the clinic, the process is a point of vulnerability and a significant percent of specialty referrals aren’t completed, in part due to missing information, misguided referrals and faulty communications.[81] [82] In the context of perinatal care, if a referral is not completed, patients may not receive needed services, which can lead to decreased quality of care, decreased patient and provider satisfaction and, ultimately, poorer health outcomes for pregnant people and their babies.[83] The National Committee for Quality Assurance (NCQA) recognizes the importance of referral networks and their management as a core component of patient-centered medical home activities.[84] Building a reliable network of service partners and processes to provide information necessary to inform referrals as well as having mechanisms to track referral results is an important part of providing coordinated care that is person-centered.
Leveraging this intervention to improve equitable health outcomes and attend to patients' social needs
A contributor to inequity in perinatal health outcomes is unequal access to services and resources to help patients with their condition.[85] The heart of this activity is to empower both the care team and patients through development and maintenance of a robust process to help patients access medical, behavioral health and community resources.
Many factors can impact whether or not a patient accesses a referral, including language, culture and lack of understanding of why referral is being requested. Lack of understanding of why a referral is being sought is often a barrier for patients to follow up with a referral, particularly if a patient is not experiencing symptoms. When appropriate, referrals for social needs and to community health programs can help address barriers, including those around transportation, language and basic needs of food and housing stability, all of which are associated with poorer health outcomes.
Action steps and roles
1. Identify types of referral partners that your practice needs and gaps in resource availability.
- Some examples to consider for perinatal care include maternal fetal medicine specialists; sites for ultrasound and other relevant imaging; cardiology; social services providers; substance use providers; and social service providers, including community-based organizations with resources to support patients experiencing homelessness, foster youth, adolescent pregnant patients, and pregnant patients with high frequencies of emergency department visits.
- Encourage close communication with Medi-Cal managed care plans, enhanced care providers or lead care managers, and community support providers.
- In areas where you have gaps in referral providers, telehealth services may be an option. For further information on telehealth services, including e-consult, synchronous, asynchronous, and e-visits, contact your managed care plan and/or refer to Telehealth Reimbursement Guide (Pages 14 to 16). Referral processes and tracking are also important to establish for telehealth as well as in-person services.
- Note that there is a shortage of behavioral health clinicians in many parts of California. As you continue to expand your network of off-site behavioral health providers to meet pressing behavioral health needs, also consider behavioral health integration strategies including expanding your practice’s capacity for providing integrated behavioral health services. See the PHMI People with Behavioral Health Conditions Guide for more about deepening and expanding integrated care.
- Work with the care teams for pregnant people to identify gaps in referral resources that could enhance implementation of evidence-based care.
- Use social health screening results that have been disaggregated by REAL and SOGI alongside patient and family feedback to identify unmet needs for which resource relationships have not been established.
2. Assess what tools would be beneficial for the core elements of your referral process.
Examples include (see resources below):
- Referral request form | Determine what information is required for the provider who is receiving the referral. Information may include the requested service, timing (urgent vs. standard), minimum necessary information, such as patient contact information and applicable demographics, and appropriate clinical and social support questions. For pregnancy-specific referrals, some specialists require additional information, such as working due date, pertinent labs and previous ultrasounds.
- Referral tracking spreadsheet or software | Information in a tracking system can include date of referral, appointment status and whether follow up is needed. Reach out to your Medi-Cal managed care plans as you are developing referral tracking processes. The MCPs are required to show that Medi-Cal patients are being connected to the services that they are eligible for and referred to; this includes preventive services, specialty services and social services. The MCP may be a good resource for tools such as those needed for tracking and reporting.
- Referral workflow diagram | A visual representation or workflow diagram can support staff in the referral process. The Institute for Healthcare Improvement (IHI)’s Closing the Loop: A Guide to Safer Ambulatory Referrals in the EHR Era provides a visual nine-step closed loop referral process for specialty referrals, as well as suggestions for improving the process.
3. Assess what tools would be beneficial in enhancing and tracking your referral process.
- Referral guidelines | For social services, positive responses to screening questions and tools may be the prompt for referral. Other types of referrals may be optimized by having documented referral guidelines, such as information needed by specialty provider in order to best answer referral questions.
- Communication templates | For high-volume or frequent referral types, a standardized template for communication between the clinic and referral staff can help ensure that that essential information is conveyed efficiently. Examples may include referral letters, progress notes and post-visit summaries of plan of care.
- Patient education materials (develop in conjunction with referral network) | Educational materials and resources for patients that explain the referral process and what to expect can enhance patient understanding and support referral completion. In addition, consider training medical assistants as well as any dedicated care coordination staff in evidence-based communication techniques, such as teach-back or motivational interviewing to leverage team-based care in supporting the patient to follow through with the referral after the visit.
- Staffing | Given the specifics of perinatal referrals, consider assigning dedicated staff to pregnancy-related referrals. This allows the staff member to cultivate relationships with specialists and ensure referrals are processed efficiently, given the time sensitivity of many perinatal referrals.
4. Develop approaches to fill resource gaps.
Suggested team member(s) responsible: Clinic leadership.
- Outreach to your managed care plan (MCP) to understand what resources are available. MCPs are required to have online provider directories, which include specialists, which can be a resource used by a clinic to help find contracted specialists near the patient's home. In addition to comprehensive networks of over a dozen core specialty providers and information on behavioral health and substance use resources, many MCPs are building links to access community based resources in addition to the 14 Medi-Cal Community Supports and extended care management teams through referral platforms that act as a hub to coordinate social needs for patients.
- Identify external providers and community resources that can serve as partners in care, and use the established referral process to fill gaps in care they can address.
- Meet and schedule time with high-volume providers, including community-based organizations, to develop a mutual understanding of goals of referrals and opportunities for development of shared processes (e.g., referral form).
- The American Academy of Pediatrics (AAP) offers a sample tool to develop a resource list.
5. Regularly review and update the referral processes and network.
Suggested team member(s) responsible: Clinic leadership.
- As new patient needs are identified, use that opportunity to identify potential resources and expand the referral network. If practices have trouble accessing a contracted specialist for their patient because of either overly long wait times or that they are no longer accepting new patients, the MCP is required to approve an out-of-network referral to a more available specialist.
- On a periodic basis, review referral tracking reports to identify referral resources that are used most frequently and use that information to reinforce the relationships and provide feedback on value.
- Review referral tracking reports to identify resources for which loop closure is lacking or from whom required information is not being received on a regular basis. Outreach to these organizations to reinforce expectations or, if necessary, identify a replacement resource for the network.
- For going deeper in tracking quality improvement metrics, practices can develop metrics to assess the effectiveness of the referral network. This might include tracking referral completion rates, patient satisfaction, and time from referral to specialist appointment.
Resources
Assessment of Community Referral Platforms
This vetting tool matrix was used by West County Health Centers (WCHC) to assess various social service referral platforms, including Aunt Bertha, WellSky. Health Leads, NowPow and One Degree.
KEY ACTIVITY #18:
Strengthen Community Partnerships
This key activity involves the following elements of person-centered population-based care: proactive patient outreach and engagement; care coordination; address social needs.
Overview
Strengthening partnerships with community-based organizations that share the practice’s vision and goals for its patient population enables the practice to provide more holistic care to patients and meet crucial patient social needs. Your practice can leverage existing community infrastructure to provide resources unavailable within the medical home. Community partners provide various services that meet patients’ basic needs, such as education, housing, food, transportation, employment assistance and social support.
This activity provides considerations and tips for strengthening partnerships, although note that deep engagement in this work can require significant resources from your practice.
Why this matters
Local social service organizations are rooted within the communities they serve; thus, they have a deep understanding of the needs and preferences of their communities, as well as local resources and challenges. They can support outreach and health literacy efforts and participate in codesign by providing insight around clinical initiatives serving particular patient populations.
Leveraging this intervention to address social health and equity
Building and strengthening relationships with community-based partners can extend the reach and impact of practices by facilitating patient access to services that the practice is unable to provide. Through partnerships with organizations that provide housing supports, nutrition assistance, transportation, and other social needs, practices can play an active role in helping to address health-related social needs. The PHMI Equity Framework and Approach should inform partnership development to ensure the work of partnership building is prioritizing community groups that experience injustice and structural violence.
Action steps and roles
1. Start by understanding the resources and partnerships available through Medi-Cal.
Suggested team member(s) responsible: Clinic operations and leadership staff who will liaise with community partners.
Resources include supports that are available to all Medi-Cal patients, such as transportation to medical appointments, as well as Medi-Cal Community Supports for eligible individuals with higher levels of social needs. The following is a list of social support resources that are available to Medi-Cal patients when eligibility criteria are met.
- Transportation to medical and other Medi-Cal-covered appointments.
- In-home supportive services, including personal home care assistance for those who qualify.
- Community-based adult services, including day programs outside the home for individuals who need assistance with activities of daily living.
For individuals with the highest needs, the 14 Medi-Cal Community Supports are:
- Housing transition navigation services.
- Housing deposits.
- Housing tenancy and sustaining services.
- Short-term post-hospitalization housing.
- Recuperative care (medical respite).
- Day habilitation programs.
- Caregiver respite services.
- Nursing facility transition and diversion to assisted living facilities.
- Community transition services and/or nursing facility transition to a home.
- Personal care and homemaker services.
- Environmental accessibility adaptations (home modifications).
- Medically supportive food and meals and medically tailored meals.
- Sobering centers.
- Asthma remediation.
For specific providers in your area, contact the provider services department of your Medi-Cal managed care plan to learn more about the providers of these services. With a list of contracted community based organizations, your practice can start to build relationships and support ongoing social needs for your patients.
For an overview of Community Supports in the state, DHCS has provided information about the current state of Enhanced Care Management and Community Supports in the Community Supports Year 1 Summary and the Enhanced Care Management Year 1 Summary.
2. Complete an environmental scan to understand who your patients identify as trusted messengers and resources in their community.
Suggested team member(s) responsible: Health center leadership, community health workers, social work staff.
- Interview patients and families.
- Learn from your community health workers.
- Confirm your existing partnership relationships.
- Develop a stakeholder map and community profile of key current and prospective partners.
- Partner with hospitals, community behavioral health centers, public health, and other key stakeholders to refine your community needs assessments.
- For pregnant people, community partners you might want to refer your patients to include organizations providing childbirth and parenting classes, midwifery practices, doula services, organizations providing breastfeeding support, home visiting programs, and the local fire and police stations, which can perform car seat checks.
3. Convene partners as a workgroup to develop strategies and interventions to address health-related social needs.
Suggested team member(s) responsible: Health center leadership.
- Serve as a convener, bringing partners together for collaboration, and don’t simply rely on individual relationships with external organizations.
- Be clear on your asks and offers to ensure the relationship will be mutually beneficial.
- Develop a shared aim statement with your partners as to why this work is important and your vision of what you hope to achieve.
- Formalize your structure and system of collaboration accountability for progress in the form of ongoing pacing of meetings on a regular basis rather than relying on transactional relationships.
- Develop memoranda of understanding clarifying expectations, roles, and commitments.
- Outline clear next steps and action items with clear roles and responsibilities to maintain accountability across partner organizations.
4. Collaborate with your partners to develop a shared set of strategies on a community approach to address health-related social needs.
Suggested team member(s) responsible: Health center leadership.
- Benchmark and collate approaches to identify potential interventions for addressing health-related social needs.
- Leverage CalAIM resources as part of your intervention plans.
- Develop a driver diagram to guide your efforts and to set priorities.
5. Collaborate with partners to collaboratively design and execute interventions and approaches to address health-related social needs.
Suggested team member(s) responsible: Health center leadership.
- Use workflow mapping tools, swim lane diagrams, and checklists that clarify roles and plan initiatives.
- Develop clear action plans clarifying leaders of intervention strategies, timetables, and measures of progress and success.
Implementation tips
- Health centers are very adept at developing relationships in the community, but may find it challenging to nurture long-term partnerships. A partnership starts with relationships, moves beyond referral for resources or support, and results in co-ownership for addressing community challenges.
- Be clear on being able to have an offer as well as ask when approaching a prospective partner. Avoid transactional relationships with community partners and ensure the partnership has value for all parties.
- Seek to understand your partner’s needs for results, data and reporting. Explore how the partnership can help your partner meet a need or resolve a pain point in their core mission.
- Reach out to your local managed care plan (MCP) to determine processes for payment and care management.
- Learn what is in place for your county through the Medi-Cal program and your managed care plans. If resources are not available, explore technologies that facilitate community referrals such as findhelp.org and Unite Us Cross-sector collaboration software.
- Going deeper in strengthening partnerships: Addressing community needs requires sustainable and effective partnerships over time. A future activity includes how your organization works with other community partners in an ongoing forum to address community needs (e.g., forming a community partner advisory committee). This often involves the health center as a backbone organization supporting a local collaboration governance structure for shared prioritization and action planning.
- On the horizon in strengthening partnerships: A mature partnership structure in a health center includes assessing the effectiveness of the partnerships and finding ways to continuously ensure alignment so that partnership remains a positive force for all participants. Where possible, making adjustments, such as improved data sharing and pooling of resources to increase leverage in the community, that strengthen the partnerships can be explored.
Resources
KEY ACTIVITY #19:
Provide Care Management
This key activity involves the following elements of person-centered population-based care: operationalize clinical guidelines; proactive patient outreach and engagement; care coordination; behavioral health integration; address social needs.
Overview
What is care management? How does it differ from care coordination?
Led by a care manager (a licensed clinician or a nonlicensed trained individual), care management is an intervention intended to support the highest-need individuals within your practice. The services are more targeted, require the development of a person-centered care plan, and are of higher intensity than care coordination services. A patient must consent to participate in care management activities. A care manager works directly with the patient and multidisciplinary care team members to identify, plan and implement person-centered goals and care. The care manager supports the individual in identifying and coordinating resources and referrals as well as supporting self-management activities to attain optimal wellness.
Why this matters
Care management provides a higher level of support to individuals who have medical, behavioral health, and/or social needs that impact their ability to access appropriate levels of care. Individuals may be receiving frequent emergency room (ER) and hospital care that could be avoided with care management activities and/or patients may have significant social barriers (housing, food and substance use) that prevent them from accessing preventative and wellness care.
Research points to care management as a potential intervention to improve outcomes for higher risk obstetric patients, such as patients at risk for preterm delivery.[86] There is a paucity of resources, however, on care management guidelines specific to the pregnant or postpartum population. Resources developed for the primary care population may need to be adjusted for the pregnant population.
Leveraging this intervention to improve equitable health outcomes and attend to patients’ social needs
Care management holistically addresses a patient’s medical, behavioral health and social health needs. Addressing health-related social needs helps in reducing health disparities among different populations. Individuals with lower socioeconomic status or limited access to resources can be provided with resources to support these areas. As part of care management, the patient’s social needs are directly addressed as part of the assessment and prioritized according to the patient's goals. For example, attaining stable housing may be the first step to achieving better health in their pregnancy.
What type of patients are eligible for care management?
Individuals eligible for care management have high levels of need in one or more of the domains of medical, social or behavioral health. Some examples of populations who may be eligible for care management include:
- Individuals with complex medical needs, also known as complex care management.
- Example: A patient with chronic hypertension and type 2 diabetes, currently pregnant with her fourth child.
- Goal of care management: Support optimal nutrition and medication management to minimize risks to pregnancy. Address social needs that may impact the pregnant person’s ability to manage their conditions, such as housing stability and food insecurity. Coordinate appointments for specialty visits with maternal fetal medicine.
- Individuals who require intensive support post hospital discharge / care transitions.
- Example: A postpartum patient who had severe preeclampsia and was hospitalized for four weeks at the end of her pregnancy. She has been discharged home, but her baby is still in the neonatal intensive care unit (NICU), and she is experiencing postpartum depression symptoms.
- Goal of care management: to coordinate counseling, medications, medical equipment (e.g., home BP cuff, hospital-grade lactation pump), follow up postpartum care to support optimal recovery and mental health, and minimize risk of rehospitalization.
CalAIM: Enhanced Care Management and Community Supports.
In California, Medi-Cal beneficiaries who experience high care management needs, may be eligible for a Medi-Cal benefit known as Enhanced Care Management or ECM. Beginning in 2024, this benefit will be available for pregnant and postpartum patients. ECM can be provided to eligible Medi-Cal beneficiaries at risk of poor outcomes due to high levels of medical, social and behavioral health needs. ECM delivers person-centered, trauma-informed care management services, and members can access additional services known as Community Supports to help achieve their medical and social health goals.
DHCS Enhanced Care Management (ECM) and Community Supports[87] are foundational parts of the transformation of Medi-Cal focused on:
- Breaking down the traditional walls of healthcare, extending beyond hospitals and healthcare settings into communities;
- Introducing a better way to coordinate care; and
- Providing high-need members with in-person care management where they live.
If your practice has many patients who are eligible for ECM based on descriptions below, you can contact your Medi-Cal managed care plan (MCP). Your MCP can provide you with details on patient eligibility and the requirements needed to provide ECM services to your patients. Some clinics also provide Community Supports services depending on their patient population.
ECM is available to specific groups of Medi-Cal members (called ECM populations of focus).[88]
- Adults, unaccompanied youth and children, and families experiencing homelessness.
- Adults, youth, and children who are at risk for avoidable hospital or emergency department care.
- Adults, youth, and children with serious mental health and/or substance use disorder needs.
- Adults living in the community and at risk for long-term care institutionalization.
- Adult nursing facility residents transitioning to the community.
- Children and youth enrolled in California Children’s Services (CCS) or CCS Whole Child Model with additional needs beyond their CCS condition(s).
- Children and youth involved in child welfare (foster care).
- Adults and youth who are transitioning from incarceration.
- Pregnant and postpartum individuals; birth equity population of focus (starting in 2024).
Medi-Cal members can also be connected to Community Supports services to help address their health-related social needs, such as access to healthy foods or safe housing to help with recovery from an illness. If your clinic wants to provide Community Supports services, contact your Medi-Cal managed care plan for information. Available Community Supports services include:
- Housing transition navigation services.
- Housing deposits.
- Housing tenancy and sustaining services.
- Short-term post-hospitalization housing.
- Recuperative care (medical respite).
- Day habilitation programs.
- Caregiver respite services.
- Personal care and homemaker services.
- Nursing facility transition or diversion to assisted living facilities.
- Community transition services or nursing facility transition to a home.
- Environmental accessibility adaptations (home modifications).
- Medically tailored meals and medically supportive food.
- Sobering centers.
- Asthma remediation.
How does an eligible individual get connected to ECM and Community Supports services?
The Medi-Cal managed care health plans are responsible for identifying their patients who are candidates for Enhanced Care Management and meet eligibility requirements. In addition, practices, providers and community-based organizations have the ability to refer patients for ECM services. Community-based organizations, such as homeless services providers, are a particularly valuable source of referrals into ECM, as they often have trusted relationships with individuals who may not have sought or received medical care and are therefore not known to the MCP because they have had little or no utilization of healthcare services.
How do we refer a patient who we think would benefit from ECM?
If you have a patient who may be a candidate for ECM or Community Supports services, you should contact the Medi-Cal managed care plan to inquire about services available through the patient’s health plan. Patients and family members can self-refer to ECM.
Action steps and roles
How can we provide care management services, including ECM services, in our practice?
Community practices are often well situated to provide care management services as they are the site where patients seek or can be connected to care. Clinics may decide that they want to provide care management services, including ECM services. The following resources can help assess your capacity to provide care management services within your clinic structure.
Care management for complex populations
A resource on starting a care management program for individuals with multiple medical, behavioral health and social needs is available from the Camden Coalition. This resource addresses the following areas:
- Program design: Tools to support the understanding and identification of a complex care population, plan a care model and workflow, and anticipate legal/business needs.
- Program operations: Tools to support the implementation of a complex care model including triage, outreach, engagement, intake and clinical support.
- Data and process improvement: Tools to support metric identification, data collection and analysis, and process improvement.
- Team and leadership development: Tools to support the recruitment, training and management of a complex care team.
- Community mapping and collaboration: Tools to support multisector and community coordination.
- Communication and growth of success: Tools to support broad communication and program scaling.
Care transitions
This Care Transitions Toolkit from the Indiana Hospital Association focuses on processes to support care management for individuals transitioning between healthcare settings.
ECM services
This DHCS Enhanced Care Management Provider Toolkit provides a detailed description of the services that are required to become an ECM provider. In this guide, the requirements of ECM providers are outlined in detail.
FIGURE 20: EXAMPLE OF HOW AN EHR CAN ASSIST WITH CARE MANAGEMENT
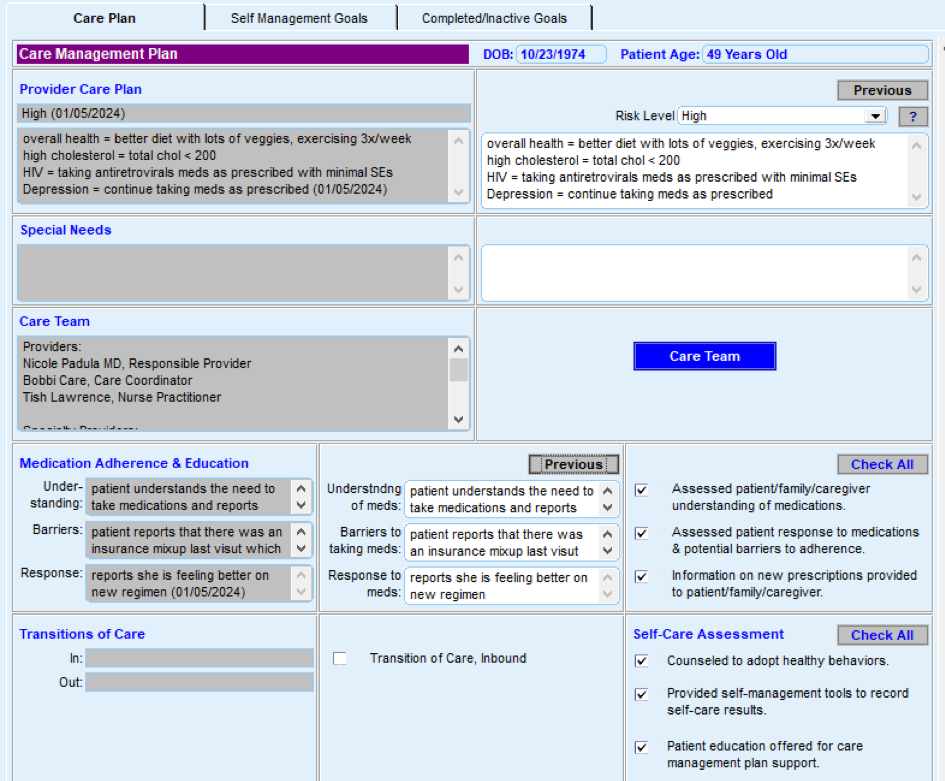
Resources
Evidence base for this activity
Chuang E, Pourat N, Haley LA, O’Masta B, Albertson E, Lu C. Integrating Health And Human Services In California’s Whole Person Care Medicaid 1115 Waiver Demonstration. Health Affairs. 2020 Apr 1;39(4):639–48.
Tomoaia-Cotisel A, Farrell TW, Solberg LI, Berry CA, Calman NS, Cronholm PF, et al. Implementation of Care Management: An Analysis of Recent AHRQ Research. Medical Care Research and Review. 2016 Oct 23;75(1):46–65.
KEY ACTIVITY #20:
Strengthen a Culture of Equity
This activity builds off of your practice's application of Key Activity 4: Use a Systematic Approach to Decrease Inequities within the Population of Focus to provide strategies and in-depth resources that can help practices create or strengthen a culture of equity in your practice. The PHMI Equity Framework and Approach emphases that achieving long-term and sustainable improvements to health and racial equity for patients and the broader ecosystem requires a transformational shift at the organizational level. The following strategies can help practices strengthen a culture of equity:
- Demonstrate senior leadership’s ownership of and commitment to improving health equity.
- Understand and address internalized, personally mediated, and institutionalized racism.
- This should include ongoing learning and development activities on the full range of health equity topics (e.g., anti-bias, structural racism, race-based algorithms).
- Build organizational capacity to support efforts to improve health equity.
- Establish practices and policies to promote workforce diversity and provide culturally and linguistically appropriate care.
- Support policy efforts to eliminate inequities driven by social drivers of health.
- This can take the form of joining advocacy efforts or supporting patients in accessing resources and services created by recent policy reforms, such as Medi-Cal Community Supports for housing or medically tailored meals. See the Key Activity 7: Use Social Needs Screening To Inform Patient Treatment Plans for a discussion on social needs.
Resources
On the Horizon Key Activities
More advanced activities that build off of the foundational activities and that help ensure your practice can achieve equitable improvement in your prenatal and postpartum care.
KEY ACTIVITY #21:
Telehealth in Perinatal Care
Overview
The modern schedule of prenatal and postpartum visits was developed almost a century ago; in this paradigm, visits occur in-person in a cadence that varies little from patient to patient. The COVID-19 pandemic presented an opportunity to reimagine perinatal care, beginning with the necessary introduction of telehealth visits to promote patient safety. This has led to efforts to better tailor schedules of prenatal and postpartum visits to meet the individualized clinical and social needs of each patient.[89] In California, many of the telehealth flexibilities implemented to respond to the public health emergency remain available[90] to patients and providers in the current state. Thoughtfully integrating telehealth into your provision of perinatal care services could be beneficial in supporting care quality, patient experience, and health equity.
Why this matters
Telehealth can serve as a useful tool to leverage in meeting many of the quality measures of interest in the perinatal population. For example, timely (first trimester) entry into prenatal care can be supported using telehealth for intake visits with intention (e.g., to guide physical examination and tailored laboratory and imaging studies prior to follow up). Depression screening can be performed via telehealth both prenatally and postpartum. Two postpartum visits are recommended for Medi-Cal beneficiaries; one of these two visits (either earlier or later) could be provided via telehealth, if aligned with the patient’s postpartum clinical needs. Beyond these specific quality-related benefits, the use of telehealth may have other advantages in providing services specific to the perinatal population[91] such as consultation with specialists, lactation support, and mental health services.
High-quality telehealth in perinatal care calls for greater patient engagement through self-monitoring. Weight, blood pressure and even fetal heart rate are key clinical data elements that patients can gather on their own. This level of engagement in care may improve patient confidence and self-efficacy in managing their own health.
Leveraging this intervention to improve equitable health outcomes
Integrating telehealth into your perinatal workflows must be done with equity at the center.[92] Failing to consider health equity in telehealth implementation can in fact worsen disparities in care access and quality. The COVID-19 pandemic demonstrated that telehealth services had to be paired with equitable patient access to hardware and broadband networks. Language and health literacy considerations must be addressed in the provision of telehealth as they would be in all clinical care.
Once the obstacles to access described above are addressed, telehealth has great potential to improve equitable health outcomes in the perinatal population.
Leveraging this intervention to attend to patients’ social needs
Subgroups of your pregnant and postpartum population with social needs may have the most to gain from the equitable integration of telehealth into your practice. Telehealth has shown to greatly benefit patients with transportation barriers (e.g., rural populations, those without vehicle access). It may also improve adherence to care among patients with competing needs, including inflexible jobs and childcare needs.
Action steps and roles
1. Identify quality gaps where telehealth could help.
Suggested staff responsibilities: Clinical lead, operations lead, data or evaluation lead.
Quality measures where telehealth might be leveraged should be identified. Data should be stratified by key sociodemographic factors to identify any patient subpopulations where the introduction of telehealth could mitigate care inequities.
2. Infrastructure: Telehealth operations and billing.
Suggested staff responsibilities: Operations lead, IT lead.
If telehealth services are new to your practice, appropriate technology and data security infrastructure must be put into place[93] prior to launch. Accurate coding and billing workflows for telehealth should also be developed.
3. Create telehealth workflows.
Suggested staff responsibilities: Clinical lead, operations lead, frontline staff, patients.
Introducing telehealth visits into your perinatal care model will impact existing standard clinical workflows. Engaging all clinical staff into redesigning these workflows will be key. Patient perspectives must be considered in launching telehealth with enough support to ensure its uptake.
KEY ACTIVITY #22:
Group Postpartum (New Parent) Care
Overview
Group postpartum care represents an opportunity to expand care and relationships established during the prenatal period. While less common than group prenatal care, group postpartum care and new parent groups within community heath settings are an emerging approach. Providing postpartum and well child care in group settings has the potential to improve the provision of care by enhancing patient/provider relationships as well as peer relationships in the postpartum period.[94]
Why this matters
Lack of community is a risk factor for postpartum depression.[95] Leveraging the group care setting for postpartum patients can provide an avenue to create more community for new parents. Group postpartum and parenting groups also increase the time patients have to interface with a healthcare provider, as group sessions are significantly longer than individual clinic visits.
Action steps and roles
1. Review group postpartum care interventions to identify which model may be appropriate for your practice and the populations it serves.
Suggested team member(s) responsible: Practice leadership, care team, financial lead, billers and coders.
CenteringParenting is the most established postpartum and well child curriculum available in the United States. It may also be more feasible for a CHC to adapt their group prenatal modality for the postpartum setting. Learn about the models through research and by speaking with other health centers or organizations that are conducting group postpartum care as well as reaching out directly to the model developer. Remember that there will be costs associated with training and certifying your practice depending upon the group prenatal care model you select to implement.
2. Assess the health center’s capacity to implement a group care model.
For the assessment, consider patient panel, provider capacity, physical space available to convene the groups, and clinicians and staff who would serve on an implementation team. Note that group postpartum visits require coordination between OB/GYN providers and pediatric providers given the overlapping content and care provided.
3. Educate clinicians and staff on group postpartum care.
Educate health center staff on the value of group care and how it will be integrated into health center care services. Ensure providers and staff have the necessary information and materials to make referrals to group prenatal care. Some group care models (e.g., CenteringPregnancy) may charge for staff training and site certification.
4. Ensure a core implementation team is available to support group postpartum care.
Establish a core implementation team, likely overlapping with group prenatal care team, with dedicated time to implement group postpartum care with fidelity. Ensure facilitators receive necessary training to create a trauma-informed and culturally responsive environment.
5. Conduct continuous quality improvement.
Solicit feedback from individuals who participated in group visits to identify opportunities for program improvement and ensure that the intervention is culturally responsive and trauma-informed. Convene group facilitators and educators for check-ins and sharing of lessons learned and strategies for engagement and group facilitation.
Evidence base for this activity
Gresh, A., Batchelder, A., Glass, N. et al. Adapting group care to the postpartum period using a human-centered design approach in Malawi. BMC Health Serv Res 23, 1098 (2023). https://doi.org/10.1186/s12913-023-10036-2.
McNeil DA, Johnston JC, der Lee GV, Wallace N (2016) Implementing CenteringParenting in Well Child Clinics: Mothers’ Nurses’ and Decision Makers’ Perspectives. J Comm Pub Health Nurs 2:134. doi:10.4172/2471-9846.1000134.
Appendices
APPENDIX A:
Sample Idealized System Diagram
WEAVING YOUR MEASUREMENT STRATEGY AND LEARNING SYSTEM INTO PRACTICE OPERATIONS
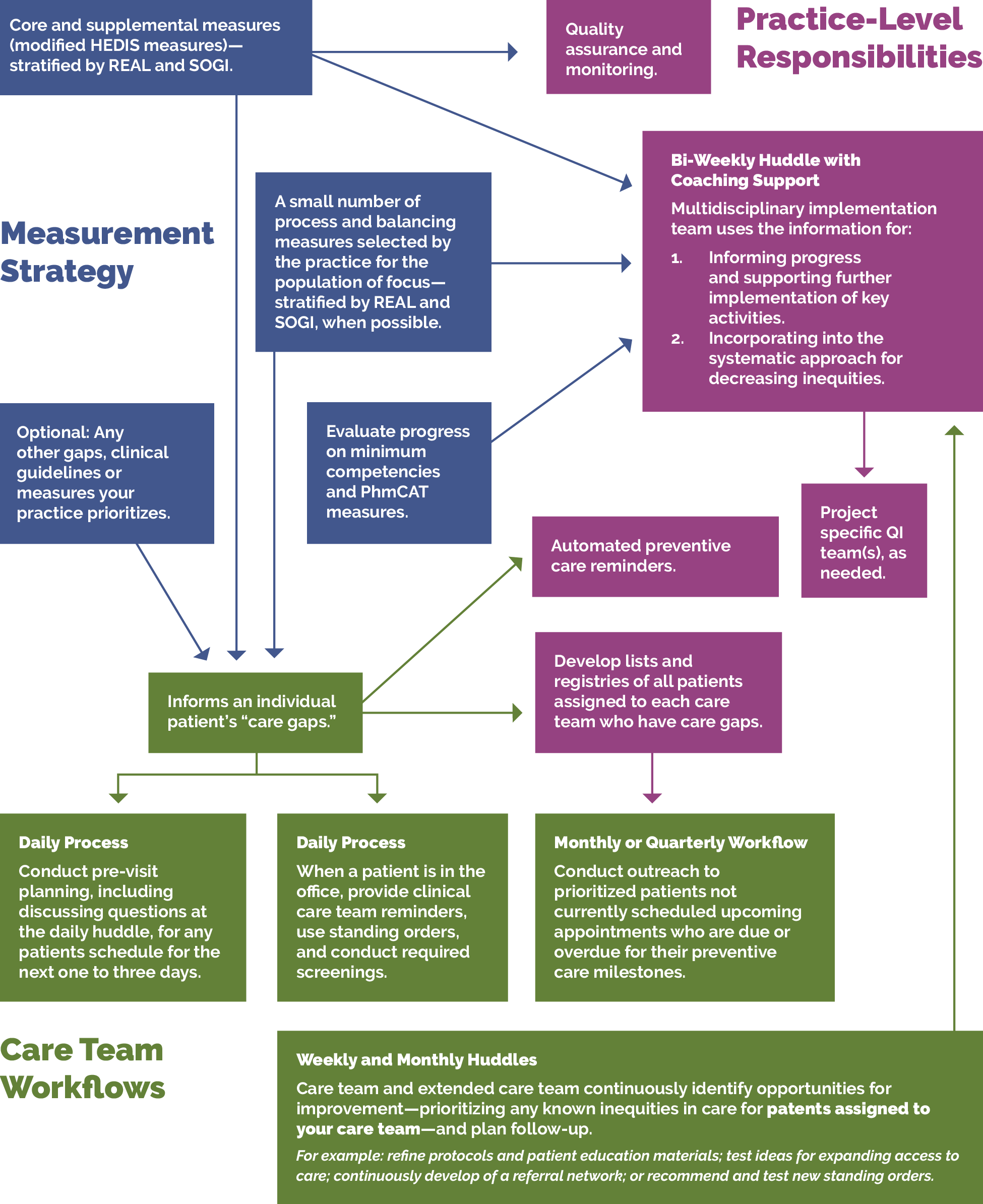
APPENDIX B:
Theory of Change
The key activities in this guide align with the PHMI theory of change for how practices can increase prenatal and postpartum visit rates through three main drivers:
- Effective implementation of prenatal and postpartum protocols.
- Patients eligible and due for care have the information, education and access needed for screening.
- Practices have needed resources and support.
FIGURE 21: PHMI PREGNANT PEOPLE GUIDE DRIVER DIAGRAM
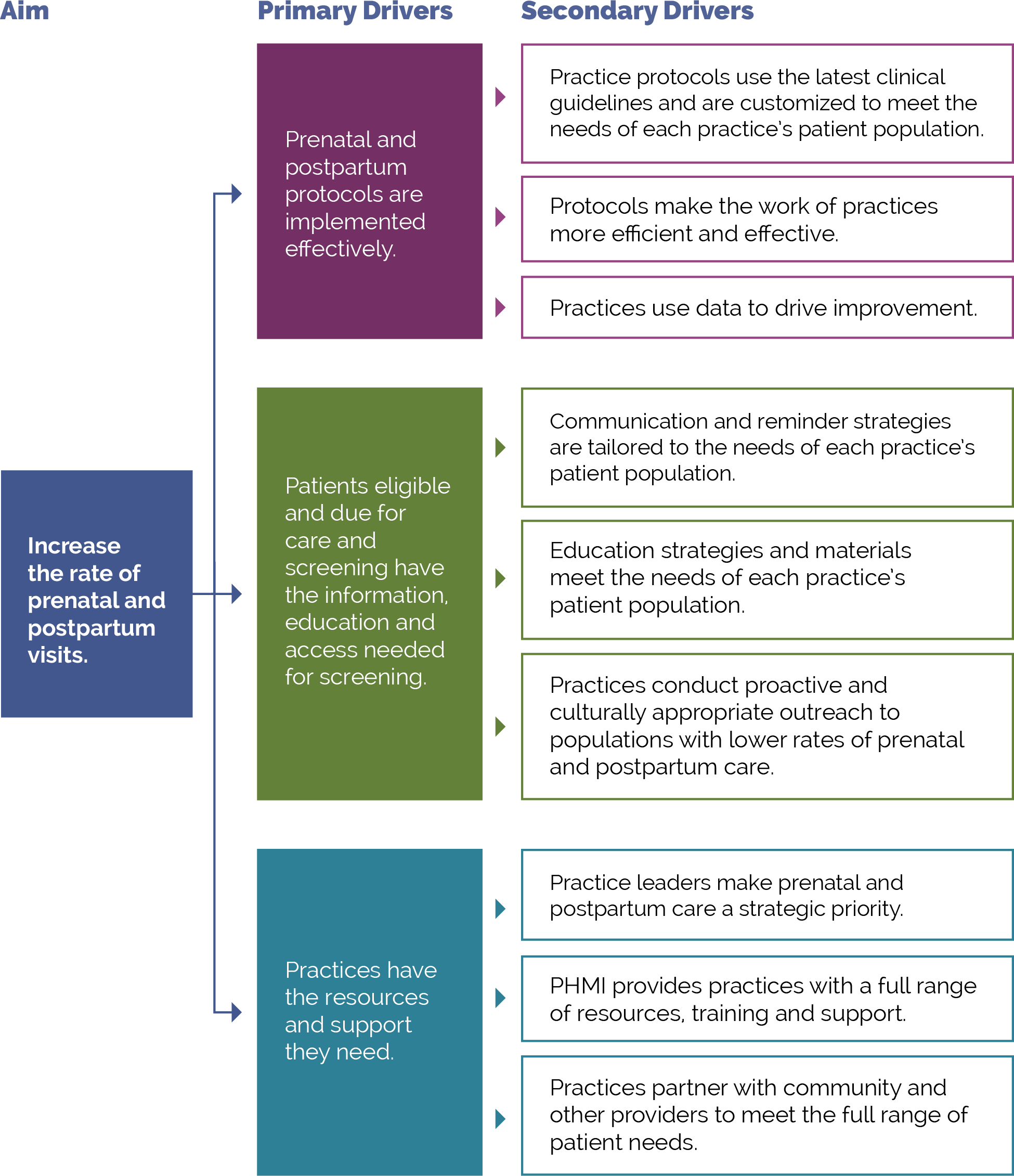
APPENDIX C:
Developing a Robust Measurement Strategy
FIGURE 22: DEVELOPING YOUR MEASUREMENT STRATEGY MILESTONES
The visual below illustrates the key milestones in the development of a robust measurement strategy.
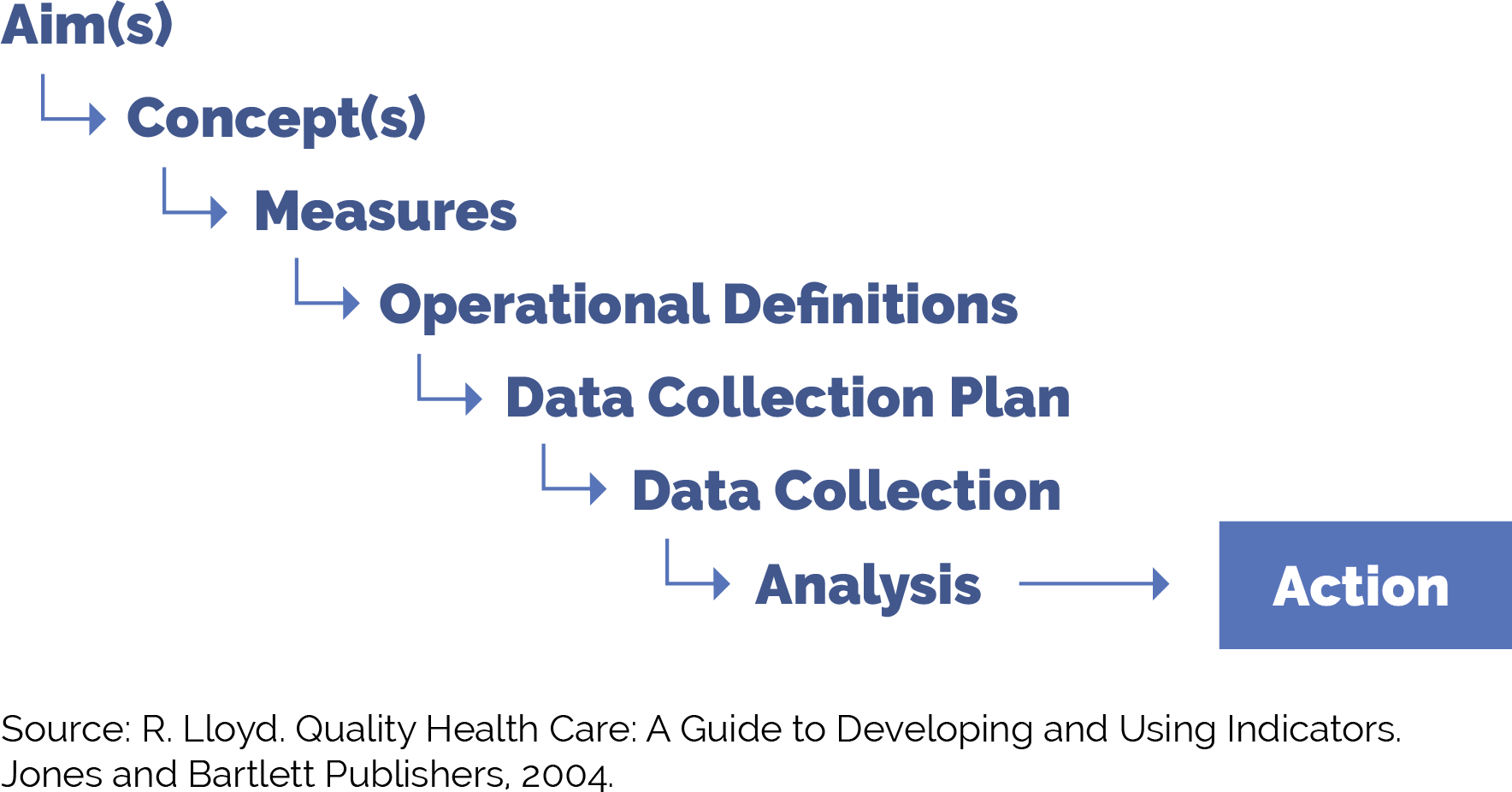
FIGURE 23: MEASUREMENT STRATEGY MILESTONES IN DETAIL
This table provides guidance on each of these milestones as you work to put in place a robust yet practical measurement strategy to improve outcomes for pregnant people.
Milestone |
Definition |
Example |
|---|---|---|
Aim(s) |
The overall goal of the improvement effort. “What are we trying to accomplish?” We often recommend sub-aims to focus your team on intermediate goals. You can develop data-informed SMARTIE goals (specific, measurable, attainable, relevant, time-based, inclusive, equitable) focused on improving specific aspects of care for attributed patients or subpopulations of patients.
|
Pregnant people will receive care that is responsive to their needs.
Example sub-aim: By December 2025, we will increase the percentage of Black pregnant people who are screened for depression while pregnant and receive documented follow-up, if positive from 52% to 100%.
|
Concept(s) |
A general, abstract notion (approach, thought, belief or perception) related to the aim of focus. |
Screening for depression is an important part of care for pregnant and postpartum people. |
Measures |
Specific objective ways to determine the extent to which an aim has been met or to determine if there has been improvement in the concepts of focus. Measures help us to answer the second question in the model for improvement: How will we know that a change is an improvement? Measures generally fall into one of three types:
|
See the “Pregnant People Sample Outcome, Process and Balancing Measures” chart later in this section. People who are pregnant and postpartum receive screening for depression and, if positive, a follow-up plan is documented (process measures). People who are pregnant and postpartum with a positive depression screen successfully complete a behavioral health follow-up (outcome measure). Wait times between a behavioral health referral and initial appointment remain stable (balancing measure). |
Operational definitions |
Detailed descriptions in quantifiable terms of what to measure and the steps to follow to do so consistently each time and over time. The operational definitions help make the measures clear and unambiguous and often contain criteria for inclusion and exclusion and numerator/denominator. |
People who are pregnant receive screening for depression and, if positive, a follow-up plan is documented: PND HEDIS. |
Data collection plan |
A detailed set of instructions that generally includes:
|
Who:
How:
Where and how the data will be stored:
When the data will be collected:
How often:
|
Analysis and action |
The process of analyzing the data, including instructions for the analysis and visualization of the data, disseminating the data to relevant parties, and using the data to track progress and guide improvement efforts. Ensure that data visualizations are easy for all frontline staff and patients to understand and engage with. |
Patient wait time analysis and action: the process where the improvement team reviews data on wait times on a weekly basis and the care team and panel manager review the data subsequently once per quarter or every six months for ongoing monitoring. |
POPULATION HEALTH GUIDE FOR UNDERTAKING 3 PART DATA REVIEW
The three part data review is a tool that can be used to advance work related to population health. It draws on asset-based inquiry, to surface to identify needs and opportunities to understand the ways in which systems have discarded or undervalued the assets of individuals and communities. Groups can then work together to ensure that all can contribute to advancing population health and well-being and dismantling inequities. Access the full resource.
APPENDIX D:
Guidance on Technological Interventions
EHRs were primarily designed to manage individual patients rather than groups of patients. However, over time, EHRs have increasingly added functionality for population-level quality reporting and management and some degree of care planning and care coordination, especially to support value-based care tracking and reporting. Practices should evaluate your EHR capabilities against specifically designed population management applications. While these applications require interface with the EHR, they generally offer additional functionality. While EHR solutions are integrated with EHR data, they still usually require import of data from outside sources to be optimally useful. Managed care organizations may provide care coordination and population management applications, usually only for their own enrolled patients. EHR-based solutions may also pose challenges where groups of practices using different EHR solutions are collaborating in value-based care contracts.
In value-based care arrangements, practices are responsible for attributed patients who may have never been seen. Since these patients do not have records in the EHR, practices need to consider how they can manage these patients to engage them into care at the practice in the absence, at least initially, of the patients having records within the EHR. If your practice is using freestanding applications for this, they need the capacity to handle these attributed patients who have not been registered as patients.
FIGURE 24: CORE POPULATION HEALTH MANAGEMENT FUNCTIONALITY REQUIREMENTS
Figure 24 includes the technical functionalities required to support population management for pregnant people. These requirements can guide the evaluation of existing solutions or guide the development of requirements in evaluating potential new applications. The table also indicates the data sources required to enable the functionality.
# |
Functionality |
Population Health Management Requirement Description |
Data Acquisition Dependency |
|---|---|---|---|
1 |
Care guidelines |
Identify care gaps for pregnant people against care protocol. Care guidelines may be presentable to clinical provider and support team at point of care through the EHR, in visit workflow as pre-visit prep and team huddle, through registries as above, and aspirationally as prompts to patients and caregivers. |
Commercial EHR embedded guidelines provided by vendor or customized by practice. External source guidelines (clinical guidelines). Reference sites made available electronically. |
2 |
Registries |
Ability to produce registries (list or cohort of patients) organized to facilitate population management: 1) Prenatal patients; 2) adults in age ranges relevant to measures and/or clinical standards; 3) adults sharing designated high-risk criteria (medical, behavioral, social needs) impacting their ability to achieve guidelines. These registries should contemplate inclusion of functionality to trigger automated, pre-defined action(s) and/or human-initiated action(s) for all or a defined subset of patients comprising the registry. Suggested HIT assets that can be leveraged to achieve this function include:
|
EHR:
External data sources, such as: reference labs, specialty care, immunization registries, and social service providers’ data. |
3 |
Clinical decision support (CDS) |
Care gaps should be displayed based on what is due with insight into previous results to support clinicians’ ability to make decisions at the point of care (POC) for the provider and care team members supporting non-POC management. Care guidelines may be presentable as clinical decision support to clinical provider and support team at point of care, in visit workflow as pre visit prep/team huddle, through registries as above, and aspirationally as prompts to patients and caregivers. While EHR based prompts are usually thought of as ideal, team-based care presents an opportunity for CDS to be presented to other members of the care team through other channels. The Five Rights Framework Clinical Decision Support: More Than Just ‘Alerts’ Tip Sheet—September 2014 is a useful guidance to help health centers to support decision-making across a wider range of the care delivery lifecycle, broader teams, and technology other than the EHR to look beyond office visits and providers. This is especially important to avoid alert fatigue and burnout. |
Internal EHR data. External source clinical data. Claims data (clinical lag should be noted). Electronic guideline specifications. Patient-contributed data. |
4 |
Care dashboards and reports |
Pregnant people dashboard: Population view by eligible study with sorting and filtering capability based on characteristics to be defined by the practice, with ability for care team and case managers to document the actions completed; ability to see care gaps at a patient level and population level according to health center-prioritized care guidelines. Note that, to automate these reports, it is necessary to apply standardized data collection strategies against electronically specified protocols. |
Same as above (EHR data and external data sources). Data from other sources of care. Claims data. |
5 |
Quality reports |
Same as above by quality measures, as opposed to care guidelines; ability to track HEDIS, as well as customized measures and uniform data system (UDS). |
Quality measure specifications. Same as above (EHR data and external data sources. Data from other sources of care. Claims data. |
6 |
Risk stratification |
Ability to categorize risk for patients and develop lists according to risk classification (tie to registry). Can be imported as externally generated risk score, or calculated internally according to proprietary or customized risk algorithm. |
Data acquisition platform ingestion is already curated. High-risk list is ingested and utilized downstream in the journey. Additional internal and external data sources to populate defined risk model. |
7 |
Outreach and engagement |
Allow for outreach to support pre-visit planning or post-visit care needs, such as assessments. Technology channels include population registry outputs and patient-facing applications, such patient portal, freestanding text messaging, and self-assessment or self-management applications. |
Same as above (clinical, EHR, etc.). Claims |
8 |
Care management |
Allow for management of specific and unique care needs for high-risk patients. Care management requires the ability for multiple members of the care team to contribute to and track elements of the plan. Challenges with freestanding care management applications include access to data from other sources of care, including the ability to track referrals, and workflow burden of staff utilizing multiple applications. Ability of the care management application to draw from and write back to the EHR is desirable but difficult to achieve. |
Care management protocols. Appointment data (internal and external). Clinical data from external service providers. |
FIGURE 25: USE OF TECHNOLOGY FOR RECOMMENDED SCREENING FOR FOUNDATIONAL KEY ACTIVITIES
This table identifies strategies for using digital tools to complete appropriate screeners as recommended by clinical guidelines. Using technology to facilitate screening may streamline the workflow and preserve patient confidentiality where necessary.
ID |
Focus Area |
Completion of Digital Screeners |
Data Acquisition Dependency |
|---|---|---|---|
1 |
Depression screening |
In-office tablet-based screening and/or remote patient-facing application-based self-completed screening.* |
Population health and EHR integration of screener responses or, at minimum, scores. |
2 |
Anxiety screening |
In-office tablet-based screening and/or remote patient-facing application-based self-completed screening.* |
Population health and EHR integration of screener responses or, at minimum, scores. |
3 |
Unhealthy substance user screening |
In-office tablet-based screening and/or remote patient-facing application-based self-completed screening.* |
Population health and EHR integration of screener responses or, at minimum, scores. |
4 |
Social needs screening |
In-office tablet-based screening and/or remote patient-facing application-based self-completed screening.* |
Population health and EHR integration of screener responses or, at minimum, scores. |
*A workflow should be codified for identifying emergent behavioral health risks. A workflow should be codified for preserving patient confidentiality.
FIGURE 26: USE OF TECHNOLOGY FOR PATIENT OUTREACH AND PRE-VISIT PLANNING FOR FOUNDATIONAL KEY ACTIVITIES
This table outlines the use of technology to facilitate specific activities and potential technology solutions that can optimize the uptake and efficiency of in-office visits.
ID |
Technology Focus |
Patient Inreach and Pre-Visit Planning |
Data Acquisition Dependency |
|---|---|---|---|
1 |
Portal-based communication |
|
EHR interface and integration. |
2 |
AI-enabled chatbots |
Identifying issues that need to be addressed before an office visit that can be converted to telehealth visits. |
Population health and EHR incorporation of screening scores and responses. |
3 |
Text messaging |
Appointment reminders. |
EHR interface and integration. |
FIGURE 27: USE OF TECHNOLOGY FOR ENHANCED PATIENT ENGAGEMENT AND VIRTUAL CARE FOR “GOING DEEPER” ACTIVITIES
The table identifies technology solutions to engage patients asynchronously from office visits for a variety of use cases to enhance care and patient experience.
ID |
Focus Area |
Patient Engagement and Mobile Technology |
Data Acquisition Dependency |
|---|---|---|---|
1 |
AI-enabled Chatbots |
|
HR interface and integration. |
2 |
Remote medical devices |
|
EHR and population health integration. |
FIGURE 28: USE OF TECHNOLOGY FOR INNOVATIONS IN CARE DELIVERY FOR “ON THE HORIZON” ACTIVITIES
The table describes technology strategies that can enhance care delivery by using artificial intelligence and advanced technology tools.
ID |
Focus Area |
Artificial Intelligence (AI) and Innovation |
Data Acquisition Dependency |
|---|---|---|---|
1 |
Predictive analytics |
|
EHR integration, population health, and patient engagement application integration. |
2 |
Artificial intelligence-enabled diagnostics |
Advanced diagnostic tools that can use imaging, audio files, and EHR data to suggest diagnoses and care management plans. |
EHR integration and population health integration |
RECOMMENDED CITATION AND ACKNOWLEDGEMENTS
Recommended citation: Deane M, Pritzker J, Batra P, Clemmons N, Baker L, Howard P, Burgess K, Donald F, Rachman F, Esmond W. Pregnant People Implementation Guide. In: Coleman K, Mital M, editors. Population Health Management Initiative Populations of Focus Implementation Guide Series. 1st ed. Oakland, CA: Kaiser Permanente; 2024.
Acknowledgments: We gratefully acknowledge the contributions of the many staff and representatives of the Institute for Healthcare Improvement (IHI), AllianceChicago, Center for Care Innovations (CCI), JSI Inc and the Center for Excellence in Primary Care at University of California, San Francisco along with Pyramid Communications and Kaiser Permanente’s Population Health Management Initiative (PHMI) team for crafting this work.
In addition, we are grateful for the partnership of the Department of Health Care Services (DHCS), Community Health Center partners in PHMI, representatives from the California Primary Care Association and the Regional Associations of California (RAC) along with the many other academic, health plan and consulting partners who shared their expertise and insights freely as we collaboratively designed the initiative and created these guides.
Special thanks to the individual reviewers of this first edition of the Populations of Focus Implementation Guide Series who significantly strengthened this work, including: Jeff Norris, David Tian, Karen Mark, Palav Babaria (DHCS); Jennifer Sayles (Pop Health Learning Center); Roger Chaufournier, Christine St. Andre (IHI); Kathleen Figoni, Angela Sherwin (CCI).
Endnotes
- Trost S et al. Pregnancy-Related Deaths: Data from Maternal Mortality Review Committees in 36 US States, 2017-2019. CDC DHHS 2022. In addition to the 2018 CDC citation.
- Centers for Disease Control and Prevention. Working Together to Reduce Black Maternal Mortality. April 2023
- United States Government Accountability Office. Maternal Health Outcomes Worsened and Disparities Persisted During the Pandemic. Highlights of GAO-23-105871, a report to congressional addressees. October 2022
- Elliott K. Main, Christy L. McCain, Christine H. Morton, Susan Holtby, et al. “Pregnancy-Related Mortality in California: Causes, Characteristics, and Improvement Opportunities,” Obstetrics and Gynecology, April 2015, https://doi.org/10.1097/aog.0000000000000746
- CDC Review to Action. (2018). Building U.S. Capacity to Review and Prevent Maternal Deaths. Report from nine maternal mortality review committees. Retrieved from https://www.cdcfoundation.org/sites/default/files/files/ReportfromNineMMRCs.pdf
- CDC Review to Action. (2018). Building U.S. Capacity to Review and Prevent Maternal Deaths. Report from nine maternal mortality review committees. Retrieved from https://www.cdcfoundation.org/sites/default/files/files/ReportfromNineMMRCs.pdf
- American College of Obstetricians and Gynecologists (ACOG). (2018). Optimizing Postpartum Care. ACOG Committee Opinion No. 736. Obstet Gynecol, 131:140-150.
- Introduction | Pregnancy and complex social factors: a model for service provision for pregnant women with complex social factors | Guidance | NICE
- Improving Health Equity: Build Infrastructure to Support Health Equity. Guidance for Health Care Organizations. Boston, Massachusetts: Institute for Healthcare Improvement; 2019. (Available at www.ihi.org)
- Centers for Disease Control and Prevention. Working together to reduce black maternal mortality [Internet]. www.cdc.gov. 2023. Available from: https://www.cdc.gov/womens-health/features/maternal-mortality.html
- Chadha N, Lim B, Kane M, Rowland B. Institute for Healing and Justice in Medicine; 2020. https://belonging.berkeley.edu/race-medicine
- REaL Data Collection Toolbox [Internet]. KHA; 2022 [cited 2023 Dec 18]. Available from:"https://www.khaquality.com/wp-content/uploads/2024/01/HQIC_REaL-Data_Collection_Toolbox.pdf
- Leubner J, Wild S. Developing Standing Orders to Help Your Team Work to the Highest Level. Fam Pract Manag. 2018 May/Jun;25(3):13-16. PMID: 29989776.
- https://cepc.ucsf.edu/standing-orders
- https://www.cdc.gov/pcd/issues/2021/20_0569.htm
- ACOG. Importance of Social Determinants of Health and Cultural Awareness in the Delivery of Reproductive Health Care [Internet]. Acog.org. 2018. Available from: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2018/01/importance-of-social-determinants-of-health-and-cultural-awareness-in-the-delivery-of-reproductive-health-care
- Alegría M, NeMoyer A, Falgàs Bagué I, Wang Y, Alvarez K. Social Determinants of Mental Health: Where We Are and Where We Need to Go. Curr Psychiatry Rep. 2018 Sep 17;20(11):95. doi: 10.1007/s11920-018-0969-9. PMID: 30221308; PMCID: PMC6181118.
- https://catalyst.nejm.org/doi/full/10.1056/CAT.19.1037
- Kaiser Permanente Research Affiliates Evidence-based Practice Center. Screening and Interventions for Social Risk Factors: A Technical Brief to Support the U.S. Preventive Services Task Force [Internet]. 2021. Available from: https://www.uspreventiveservicestaskforce.org/uspstf/sites/default/files/inline-files/Social%20Risk%20Factors%20Tech%20Brief_Assembled%20for%20Web_Sep%202021_1.pdf
- Rojas L, Project S. Accountable Health Communities (AHC) Model Evaluation Second Evaluation Report RTI Point of Contact [Internet]. 2023 [cited 2024 Jan 16]. Available from: https://www.cms.gov/priorities/innovation/data-and-reports/2023/ahc-second-eval-rpt
- Sınger A, Coleman K, Mahmud A, Holden E, Stefanik-Guizlo K. Assessing the Feasibility of an Empathic Inquiry Approach to Social Needs Screening in 10 Federally Qualified Health Centers. The Permanente Journal. 2023 Dec 15;27(4):136–42.
- Byhoff E, Gottlieb LM. When There Is Value in Asking: An Argument for Social Risk Screening in Clinical Practice. Ann Intern Med. 2022;175(8):1181-1182. doi:10.7326/M22-0147
- Dassau E, Atlas E, Phillip M. Closing the loop. International Journal of Clinical Practice. 2011 Feb;65:20–5. Available at https://www.cms.gove/priorities/innovation/files/x/tcpi-san-pp-loop.pdf
- Gavin, L.. Moskosky,S., Carter, M., et al. Providing Quality Family Planning Services Recommendations of CDC and the U.S. Office of Population Affairs. MMWR 2014;63(No.4) https://opa.hhs.gov/sites/default/files/2020-10/providing-quality-family-planning-services-2014_1.pdf&sa=D&source=docs&ust=1698619531900258&usg=AOvVaw3-09xEm3H3GcRyj-bnBDQq
- Dehlendorf, Christine MD, MAS; Akers, Aletha Y. MD, MPH; Borrero, Sonya MD, MS; Callegari, Lisa S. MD, MPH; Cadena, Denicia BA; Gomez, Anu Manchikanti PhD; Hart, Jamie PhD; Jimenez, Laura; Kuppermann, Miriam PhD, MPH; Levy, Barbara MD; Lu, Michael C. MD, MS; Malin, Kiko MPH, MSW; Simpson, Monica; Verbiest, Sarah DrPH; Yeung, Miriam MPA; Crear-Perry, Joia MD. Evolving the Preconception Health Framework: A Call for Reproductive and Sexual Health Equity. Obstetrics & Gynecology 137(2):p 234-239, February 2021. | DOI: 10.1097/AOG.0000000000004255
- Reproductive Health National Training Center. Preconception Health Toolkit. https://rhntc.org/resources/preconception-health-toolkit%23assessprog&sa=D&source=docs&ust=1698619531896866&usg=AOvVaw0TZiLyyoM-vB2qZHrI610Z
- Centers for Disease Control and Prevention. Preconception Health and Health Care Is Important For All https://cdc.gov/preconception/overview.html
- Healthy People 2030. Family Planning. https://health.gov/healthypeople/objectives-and-data/browse-objectives/family-planning&sa=D&source=docs&ust=1698619531898600&usg=AOvVaw1957CRBeIDezLf90-94IsE
- Dude AM, Schueler K, Schumm LP, Murugesan M, Stulberg DB. Preconception care and severe maternal morbidity in the United States. American Journal of Obstetrics & Gynecology MFM [Internet]. 2022 Mar 1 [cited 2022 Nov 11];4(2). Available from: https://www.ajogmfm.org/article/S2589-9333(21)00245-7/fulltext
- Verbiest, S., Frayne, D., McClain, E., Woodward, S. Preconception Health and Health Care Initiative. Women’s Health Practice Bulletin 2020 https://beforeandbeyond.org/wp-content/uploads/2021/02/phc-bulletin-0223211.pdf&sa=D&source=docs&ust=1698619531907693&usg=AOvVaw2KbKsCEHuY37mrI15cbFUq
- Johnson, K.,, Posner,SF., Biermann, J., et al. Recommendations to Improve Preconception Health and Health Care --- United States A Report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. MMWR 2006. 55(RR06);1-23 https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5506a1.htm
- Power to Decide. One Key Question
- Reproductive Health National Training Center. Establishing and Providing Effective Referrals for Clients: A Toolkit for Family Planning Providers.
- Improving Postpartum Care https://www.medicaid.gov/medicaid/quality-of-care/quality-improvement-initiatives/maternal-infant-health-care-quality/postpartum-care/index.html
- The California Pregnancy Mortality Surveillance System [Internet]. www.cdph.ca.gov. Available from: https://www.cdph.ca.gov/Programs/CFH/DMCAH/Pages/CA-PMSS.aspx
- Maternal Mental Health [Internet]. Ca.gov. 2019. Available from: https://www.cdph.ca.gov/Programs/CFH/DMCAH/Pages/Communications/Maternal-Mental-Health.aspx
- The American College of Obstetricians and Gynecologists. Optimizing Postpartum Care [Internet]. www.acog.org. 2018. Available from: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2018/05/optimizing-postpartum-care
- Interpregnancy Care [Internet]. www.acog.org. Available from: https://www.acog.org/clinical/clinical-guidance/obstetric-care-consensus/articles/2019/01/interpregnancy-care
- Romano M, Cacciatore A, Giordano R, La Rosa B. Postpartum period: three distinct but continuous phases. J Prenat Med. 2010 Apr;4(2):22-5. PMID: 22439056; PMCID: PMC3279173.
- Pregnancy-Related Mortality — 2018–2020 [Internet]. www.cdph.ca.gov. [cited 2024 Jan 2]. Available from: https://www.cdph.ca.gov/Programs/CFH/DMCAH/Pages/Health-Topics/Pregnancy-Related-Mortality.aspx
- Reproductive Health National Training Center. Establishing and Providing Effective Referrals for Clients: A Toolkit for Family Planning Providers
- Reproductive Health National Training Center. Establishing and Providing Effective Referrals for Clients: A Toolkit for Family Planning Providers
- Reproductive Health National Training Center. Establishing and Providing Effective Referrals for Clients: A Toolkit for Family Planning Providers
- Reproductive Health National Training Center. Establishing and Providing Effective Referrals for Clients: A Toolkit for Family Planning Providers
- ACOG Committee Opinion Number 736: Optimizing Postpartum Care. May 2018
- O'Brien, O. A., Lindsay, K. L., McCarthy, M., McGloin, A. F., Kennelly, M., Scully, H. A., & McAuliffe, F. M. (2017). Influences on the food choices and physical activity behaviours of overweight and obese pregnant women: A qualitative study. Midwifery, 47, 28–35. https://doi.org/10.1016/j.midw.2017.02.003
- Hibbard JH, Greene J. What the evidence shows about patient activation: better health outcomes and care experiences; fewer data on costs. Health Aff (Millwood). 2013 Feb;32(2):207-14. doi: 10.1377/hlthaff.2012.1061. PMID: 23381511.
- Implementing Perinatal Mental Health Screening [Internet]. www.acog.org. [cited 2023 Dec 21]. Available from: https://www.acog.org/programs/perinatal-mental-health/implementing-perinatal-mental-health-screening#:~:text=ALL%20perinatal%20women%20should%20be%20screened%20for%20mental
- Masters GA, Hugunin J, Xu L, et al. Prevalence of bipolar disorder in perinatal women: a systematic review and meta-analysis. The Journal of Clinical Psychiatry. 2022;83(5):21r14045. doi:10.4088/JCP.21r14045
- Fawcett EJ, Fairbrother N, Cox ML, White IR, Fawcett JM. The prevalence of anxiety disorders during pregnancy and the postpartum period: a multivariate bayesian meta-analysis. The Journal of Clinical Psychiatry. 2019;80(4):18r12527. doi:10.4088/JCP.18r12527
- isner KL, Sit DKY, McShea MC, et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screenpositive depression findings. JAMA Psychiatry. 2013;70(5):490-498. doi:10.1001/jamapsychiatry.2013.87
- Cox EQ, Sowa NA, Meltzer-Brody SE, Gaynes BN. The perinatal depression treatment cascade: baby steps toward improving outcomes. The Journal of Clinical Psychiatry. 2016;77(9):1189-1200. doi:10.4088/JCP.15r10174
- Byatt N, Levin LL, Ziedonis D, Moore Simas TA, Allison J. Enhancing participation in depression care in outpatient perinatal care settings: a systematic review. Obstetrics and Gynecology. 2015;126(5):1048-1058. doi:10.1097/AOG.0000000000001067
- McLean SM, Booth A, Gee M, Salway S, Cobb M, Bhanbhro S, Nancarrow SA. Appointment reminder systems are effective but not optimal: results of a systematic review and evidence synthesis employing realist principles. Patient Prefer Adherence. 2016 Apr 4;10:479-99. doi: 10.2147/PPA.S93046. PMID: 27110102; PMCID: PMC4831598.
- Perron NJ, Dao MD, Kossovsky MP, Miserez V, Chuard C, Calmy A, Gaspoz JM. Reduction of missed appointments at an urban primary care clinic: a randomised controlled study. BMC Fam Pract. 2010 Oct 25;11:79. doi: 10.1186/1471-2296-11-79. PMID: 20973950; PMCID: PMC2984453.
- McLean SM, Booth A, Gee M, Salway S, Cobb M, Bhanbhro S, Nancarrow SA. Appointment reminder systems are effective but not optimal: results of a systematic review and evidence synthesis employing realist principles. Patient Prefer Adherence. 2016 Apr 4;10:479-99. doi: 10.2147/PPA.S93046. PMID: 27110102; PMCID: PMC4831598.
- Prenatal Care [Internet]. www.acog.org. 2021. Available from: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2018/03/group-prenatal-care
- Reproductive Health National Training Center. Establishing and Providing Effective Referrals for Clients: A Toolkit for Family Planning Providers.
- Reproductive Health National Training Center. Establishing and Providing Effective Referrals for Clients: A Toolkit for Family Planning Providers.
- Reproductive Health National Training Center. Establishing and Providing Effective Referrals for Clients: A Toolkit for Family Planning Providers.
- Reproductive Health National Training Center. Establishing and Providing Effective Referrals for Clients: A Toolkit for Family Planning Providers.
- Baass M, Newsom G. Available from: https://www.dhcs.ca.gov/formsandpubs/Documents/MMCDAPLsandPolicyLetters/APL2022/APL22-031-Doula-Services.pdf
- Baass M. RECOMMENDATION FOR DOULA SERVICES FOR PREGNANT AND POST-PARTUM MEDI-CAL MEMBERS [Internet]. [cited 2024 Jan 5]. Available from: https://www.dhcs.ca.gov/services/medi-cal/Documents/Medi-Cal-Doula-Standing-Recommendation.pdf
- Bohren MA;Hofmeyr GJ;Sakala C;Fukuzawa RK;Cuthbert A; Continuous support for women during childbirth [Internet]. U.S. National Library of Medicine; [cited 2024 Jan 15]. Available from: https://pubmed.ncbi.nlm.nih.gov/28681500/
- https://www.commonwealthfund.org/publications/issue-briefs/2021/mar/community-models-improve-maternal-outcomes-equity
- https://healthlaw.org/doulamedicaidproject/
- https://www.michigan.gov/mdhhs/keep-mi-healthy/maternal-and-infant-health/mdhhs-doula-initiative
- https://www.michigan.gov/mdhhs/-/media/Project/Websites/mdhhs/Assistance-Programs/Medicaid-BPHASA/2022-Bulletins/Final-Bulletin-MMP-22-47-Doula.pdf?rev=b6f3efcea2d641c2bb0075a901257a8f&hash=CBB0F80E0519EB878E5B36AE1D2EBBCF
- https://nonprofitquarterly.org/race-and-health-and-doulas-for-social-justice/
- Pregnancy Guidelines and Recommendations by Vaccine [Internet]. 2020. Available from: https://www.cdc.gov/vaccines-pregnancy/hcp/vaccination-guidelines/?CDC_AAref_Val=https://www.cdc.gov/vaccines/pregnancy/hcp-toolkit/guidelines.html
- ACOG Practice Advisory: “COVID-19 Vaccination Considerations for Obstetric-Gynecologic Care” (2020)
- ACOG Practice Advisory: “Maternal Respiratory Syncytial Virus Vaccination” (2023)
- Adult Immunization Status [Internet]. NCQA. Available from: https://wpcdn.ncqa.org/www-prod/05.-AIS-E-COVID-19-Indicator.pdf
- Adult Immunization Status [Internet]. NCQA. Available from: https://wpcdn.ncqa.org/www-prod/05.-AIS-E-COVID-19-Indicator.pdf
- 2023. COVID-19 Cases, Deaths, and Vaccinations by Race/Ethnicity as of Winter 2022 [Internet]. KFF. 2023. Available from: https://www.kff.org/coronavirus-covid-19/issue-brief/covid-19-cases-deaths-and-vaccinations-by-race-ethnicity-as-of-winter-2022/
- Office USGA. Maternal Health: Outcomes Worsened and Disparities Persisted During the Pandemic [Internet]. www.gao.gov. 2022. Available from: https://www.gao.gov/products/gao-23-105871
- Ghaswalla P, Poirrier JEM, Packnett ER, Irwin DE, Gray SR, Buck PO. Maternal Immunization in the U.S.: A Nationwide Retrospective Cohort Study. American Journal of Preventive Medicine. 2019 Sep;57(3):e87–93.
- Flu, Tdap, and COVID-19 Vaccination Coverage Among Pregnant Women – United States, April 2022 | FluVaxView | Seasonal Influenza (Flu) | CDC [Internet]. www.cdc.gov. 2022. Available from: https://www.cdc.gov/fluvaxview/coverage-by-season/pregnant-april-2022.html?CDC_AAref_Val=https://www.cdc.gov/flu/fluvaxview/pregnant-women-apr2022.htm
- Lacy L, Solosi I. Addressing the Social Determinants of Health May Help Increase COVID-19 Vaccine Uptake [Internet]. Urban Institute. 2022. Available from: https://www.urban.org/urban-wire/addressing-social-determinants-health-may-help-increase-covid-19-vaccine-uptake
- Business - Webflow HTML website template [Internet]. www.healthyplacesindex.org. Available from: https://www.healthyplacesindex.org/
- Weiner M, Perkins AJ, Callahan CM. Errors in completion of referrals among older urban adults in ambulatory care. J Eval Clin Pract. 2010;16(1):76-81. doi:10.1111/j.1365-2753.2008.01117.x
- Mehrotra A, Forrest CB, Lin CY. Dropping the baton: specialty referrals in the United States. Milbank Q. 2011;89(1):39–68. doi: 10.1111/j.1468-0009.2011.00619.x.
- Mehrotra A, Forrest CB, Lin CY. Dropping the baton: specialty referrals in the United States. Milbank Q. 2011;89(1):39–68. doi: 10.1111/j.1468-0009.2011.00619.x.
- https://www.ncqa.org/programs/health-care-providers-practices/patient-centered-medical-home-pcmh/
- Cai C, Gaffney A, McGregor A, Woolhandler S, Himmelstein DU, McCormick D, et al. Racial and ethnic disparities in outpatient visit rates across 29 specialties. JAMA Internal Medicine. 2021 Nov 1;181(11):1525. doi:10.1001/jamainternmed.2021.3771
- Garite TJ, Manuck TA. Should case management be considered a component of obstetrical interventions for pregnancies at risk of preterm birth? American Journal of Obstetrics and Gynecology [Internet]. 2023 Apr 1 [cited 2024 Jan 16];228(4):430–7. Available from: https://pubmed.ncbi.nlm.nih.gov/36130634/
- https://www.dhcs.ca.gov/CalAIM/ECM/Pages/Home.aspx
- https://www.dhcs.ca.gov/CalAIM/Documents/CalAIM-ECM-a11y.pdf
- Redesigning Prenatal Care Initiative [Internet]. www.acog.org. Available from: https://www.acog.org/programs/redesigning-prenatal-care-initiative
- Telehealth [Internet]. www.dhcs.ca.gov. Available from: https://www.dhcs.ca.gov/provgovpart/Pages/Telehealth.aspx
- Weigel G, Frederiksen B. Telemedicine and Pregnancy Care [Internet]. The Henry J. Kaiser Family Foundation. 2020. Available from: https://www.kff.org/womens-health-policy/issue-brief/telemedicine-and-pregnancy-care/
- Health equity in telehealth | Telehealth.HHS.gov [Internet]. telehealth.hhs.gov. [cited 2024 Jan 16]. Available from: https://telehealth.hhs.gov/providers/health-equity-in-telehealth?gclid=Cj0KCQiAkeSsBhDUARIsAK3tiec6KfLZ9Ua5_IC9WkI_E-SZfbdjBX5gtrnP4bQCmDF1GQ39P1WSjcMaAqIMEALw_wcB"
- Implementing Telehealth in Practice [Internet]. www.acog.org. 2020. Available from: https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2020/02/implementing-telehealth-in-practice
- Gresh A, Batchelder A, Glass N, Mambulasa J, Esnath Kapito, MacDonald A, et al. Adapting group care to the postpartum period using a human-centered design approach in Malawi. BMC Health Services Research. 2023 Oct 14;23(1).
- Cho H, Lee K, Choi E, Cho HN, Park B, Suh M, et al. Association between social support and postpartum depression. Scientific Reports [Internet]. 2022 Feb 24 [cited 2022 Mar 9];12(1):3128. Available from: https://www.nature.com/articles/s41598-022-07248-7